
Anterior approach to the elbow can be successfully used for open reduction of Jeffery fracture, along with continuous traction and use of skin hook, although it carries the risk of avascular necrosis of the radial head.
Dr. Sameer Desai, Department of Orthopedic, KEM Hospital, Pune, Maharashtra, India. E-mail: doctorsamdesai@yahoo.co.in
Introduction: Fractures of the radial neck are very uncommon in children, accounting for 5–8.5% of all fractures around the elbow in children, and are sometimes found with dislocation of the elbow joint. Jeffery carefully studied and classified these types of radial neck fractures with displaced radial head into several types. Very few cases with Jeffrey fractures are reported in the literature, and most cases were treated by surgery. Only one case of successful closed reduction and cast and two cases of closed reduction and percutaneous pinning have been reported.
Case Report: We report two cases of Jeffery Type 2 fractures treated by an open reduction in an 11-year-old and a 13-year-old boy. We describe the difficulties faced in the reduction of the fracture and the complications that occurred in the patients.
Conclusion: Jeffery Type 2 fracture is an uncommon and difficult-to-treat injury with the possible complication of the radial head being turned upside down if treated conservatively. Therefore, prompt recognition and careful reduction are essential in this type of injury.
Keywords: Jeffery fracture, elbow dislocation, radial neck fracture, pediatric elbow.
Fractures of the radial neck are very uncommon in children. The incidence of these fractures is only 1% of all pediatric fractures and accounts for 5%–10% of all fractures around the elbow in children [1]. The postulated mechanism is a fall with valgus loading of the elbow, leading to a fracture of the radial neck, which may be accompanied by radial head dislocation [2, 3] Jeffery classified these fractures on the basis of the displacement of the epiphysis of the radial head: [4] Type 1 is the lateral inclination from 0 to 90° due to valgus overload. Type 2 is the rotation of the epiphysis by 90° posteriorly. This is the rarest form of injury that occurs on trying to reduce a subluxation or dislocation of the elbow. This type of injury occurs as a result of the capitellum striking the anterior edge of the radial head, causing the epiphysis of the radial head to rotate posteriorly. Jeffery has compared this mechanism of injury to that of a bottle opener. Newman described the third type, in which the epiphysis of the radial head is displaced anteriorly during posterior elbow dislocation. [5] The displacement, angulation, and comminution of the fracture, as well as the patient’s skeletal maturity, govern the modality of treatment for radial neck fractures. Non-displaced and uncomminuted fractures with an angle <30° and an intact periosteum can be managed by closed reduction and a cast [6, 7]. On reviewing the literature, we found only one case of closed reduction of a Type 2 Jeffery fracture. We report two cases of surgical treatment of Type 2 Jeffrey’s fracture with good clinical results and review the literature on this difficult-to-treat injury.
Case 1 involved a 13-year-old male (Patient 1) and Case 2 an 11-year-old male child (Patient 2) who presented to the emergency department after falling on their left and right sides, respectively. The patient complained of a painful and swollen elbow with restriction of movement. At the time of presentation, the elbow was not dislocated and distal neurovascular status was normal. Anteroposterior and lateral view radiographs showed Jeffery Type 2 lesions in both patients (Fig. 1a, 1b, Fig. 2 and 3).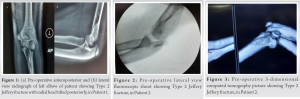 Both patients were managed similarly. Closed reduction of the fracture was tried under anesthesia but failed, so an open reduction was planned in the same setting. Using Kocher’s lateral approach, an incision was made starting from the lateral humeral condyle and curving to the radial head. The lateral collateral ligament was found to be normal. The radial head was stuck in the joint, and linear traction was given to distract the joint (Fig. 4).
Both patients were managed similarly. Closed reduction of the fracture was tried under anesthesia but failed, so an open reduction was planned in the same setting. Using Kocher’s lateral approach, an incision was made starting from the lateral humeral condyle and curving to the radial head. The lateral collateral ligament was found to be normal. The radial head was stuck in the joint, and linear traction was given to distract the joint (Fig. 4).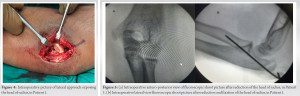 A skin hook and K-wire were used to joystick the radial head. After the radial head was reduced, it was found to be stable under fluoroscopy. We inserted a K-wire to achieve further stability (Fig. 5a, 5b and 6).
A skin hook and K-wire were used to joystick the radial head. After the radial head was reduced, it was found to be stable under fluoroscopy. We inserted a K-wire to achieve further stability (Fig. 5a, 5b and 6).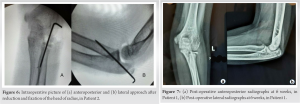 The patient was immobilized in an above-elbow slab. Postoperatively, posterior interosseous nerve function was intact. At the 6-month follow-up, Patient 1 achieved full flexion with temporarily limited extension (10°) of the affected elbow, and Patient 2 regained full movement (Fig. 7a, b, 8a, 8b, 9a, 9b, 10a, 10b). However, supination and pronation of the forearm were complete in both patients. Both children were able to continue all daily activities and participate in sports with ease at 1 year.
The patient was immobilized in an above-elbow slab. Postoperatively, posterior interosseous nerve function was intact. At the 6-month follow-up, Patient 1 achieved full flexion with temporarily limited extension (10°) of the affected elbow, and Patient 2 regained full movement (Fig. 7a, b, 8a, 8b, 9a, 9b, 10a, 10b). However, supination and pronation of the forearm were complete in both patients. Both children were able to continue all daily activities and participate in sports with ease at 1 year.
Radial neck fractures are uncommon in children. Jeffery [4] studied 450 radial head fractures, of which he included 24 rare cases in his study. Twenty-two cases were Type 1 injuries and only two were Type 2 injuries. He suggested that Type 2 injuries are rare and are caused by a mechanism similar to that of the bottle opener. To diagnose a Jeffrey Type 2 fracture before the age of five, when ossification of the radial head has not occurred, is challenging. [6] Therefore, soft-tissue shadows such as a fat pad sign require additional investigation such as ultrasound, arthrography, or magnetic resonance imaging. The interposition of the capitellum under the head and above the radial metaphysis rather than a complete dislocation is also suggestive of a Jeffrey Type 2 mechanism. Capitellum interposition leads to the failure of closed manipulation methods and further to the inversion of the radial head. Therefore, open-reduction techniques are used by many authors [6, 8]. Jeffery Type 2 fractures can present in the emergency department in two ways [4, 9]. It may be having a posterior dislocation of the elbow initially, along with a fracture of the radial neck with capitellum interposition and closed reduction is not possible either spontaneously or by manipulation. It may also present as just the fracture of the radial neck, with 90° posterior tilt of the head, without dislocation or a spontaneously reduced dislocation [10] Both these stages of the same mechanism of injury need to be identified promptly. In a series of 22 cases by Chotel et al. [6] and two cases by Wood [8], nine patients had 180° inversion of the radial head with a radiographic picture of an apparently well-reduced fracture, and five cases were found to persist after reduction with a rotation posteriorly, of at least 90°. They used open reduction for the treatment. Two were fixed with Kirschner wires, one with absorbable sutures, and the remaining two were treated in a cast only. In another patient series, the inverted radial head was put in a cast or fixed upside down because the lesion could not be identified, resulting in worse outcomes [6, 8, 11]. The treatment remains controversial and the incidence of unsatisfactory results ranges from 15% to 33%. [2] Evans and Graham [12] in their study of radial neck fractures showed that if the angulation of the fractured fragment is 60° or more, closed reduction is unsuccessful. In a study by Metaizeau et al. [13], poor results were also found to be related to the initial angle of inclination and associated forearm fractures, which require perfect reduction to prevent further periosteal, physeal, and vascular injuries. Most authors recommend immediate open reduction for these fractures. Chotel et al. performed a percutaneous reduction with Kirschner wire using an intact posterior periosteal hinge. He also recommended immediate open reduction if the closed method failed, and described the risk of damage to the articular surface with open reduction. [14] The closed reduction method involves extension and adduction of the affected elbow and digital pressure upward and inward at the most laterally prominent part of the elbow. Complications associated with this injury are avascular necrosis, growth arrest, or overgrowth of the radial head, and toppling of the radial head due to closed reduction maneuvers [15]. However, the radial head cannot be sacrificed in children and should be replaced for good results [6].
Twenty-two cases were Type 1 injuries and only two were Type 2 injuries. He suggested that Type 2 injuries are rare and are caused by a mechanism similar to that of the bottle opener. To diagnose a Jeffrey Type 2 fracture before the age of five, when ossification of the radial head has not occurred, is challenging. [6] Therefore, soft-tissue shadows such as a fat pad sign require additional investigation such as ultrasound, arthrography, or magnetic resonance imaging. The interposition of the capitellum under the head and above the radial metaphysis rather than a complete dislocation is also suggestive of a Jeffrey Type 2 mechanism. Capitellum interposition leads to the failure of closed manipulation methods and further to the inversion of the radial head. Therefore, open-reduction techniques are used by many authors [6, 8]. Jeffery Type 2 fractures can present in the emergency department in two ways [4, 9]. It may be having a posterior dislocation of the elbow initially, along with a fracture of the radial neck with capitellum interposition and closed reduction is not possible either spontaneously or by manipulation. It may also present as just the fracture of the radial neck, with 90° posterior tilt of the head, without dislocation or a spontaneously reduced dislocation [10] Both these stages of the same mechanism of injury need to be identified promptly. In a series of 22 cases by Chotel et al. [6] and two cases by Wood [8], nine patients had 180° inversion of the radial head with a radiographic picture of an apparently well-reduced fracture, and five cases were found to persist after reduction with a rotation posteriorly, of at least 90°. They used open reduction for the treatment. Two were fixed with Kirschner wires, one with absorbable sutures, and the remaining two were treated in a cast only. In another patient series, the inverted radial head was put in a cast or fixed upside down because the lesion could not be identified, resulting in worse outcomes [6, 8, 11]. The treatment remains controversial and the incidence of unsatisfactory results ranges from 15% to 33%. [2] Evans and Graham [12] in their study of radial neck fractures showed that if the angulation of the fractured fragment is 60° or more, closed reduction is unsuccessful. In a study by Metaizeau et al. [13], poor results were also found to be related to the initial angle of inclination and associated forearm fractures, which require perfect reduction to prevent further periosteal, physeal, and vascular injuries. Most authors recommend immediate open reduction for these fractures. Chotel et al. performed a percutaneous reduction with Kirschner wire using an intact posterior periosteal hinge. He also recommended immediate open reduction if the closed method failed, and described the risk of damage to the articular surface with open reduction. [14] The closed reduction method involves extension and adduction of the affected elbow and digital pressure upward and inward at the most laterally prominent part of the elbow. Complications associated with this injury are avascular necrosis, growth arrest, or overgrowth of the radial head, and toppling of the radial head due to closed reduction maneuvers [15]. However, the radial head cannot be sacrificed in children and should be replaced for good results [6].
The Jeffery lesion must be recognized promptly with due suspicion kept in mind in case of such injuries. Manipulation is often not helpful and many authors prefer open reduction. This rare injury in childhood presents a pitfall for closed reduction and may result in permanent restriction of forearm rotation. Every posterior elbow dislocation in children should be suspected and carefully evaluated with high-quality radiographs for a radial neck injury and Jeffery Type 2 fracture to avoid poor outcomes and elbow stiffness.
Jeffery fracture needs to be recognized promptly on radiographs and accurate reduction is required for good results, and surgical treatment is more successful in these cases.
References
- 1.Eilert R, Erikson M. Fractures of the proximal radius and ulna. In: Beaty J, Kasser J, editors. Rockwood and Wilkins’ Fractures in Children. 6th ed. Philadelphia: Lippincott Williams and Wilkins; 2006. p. 443-90. [Google Scholar]
- 2.D’souza S, Vaishya R, Klenerman L. Management of radial neck fractures in children: A retrospective analysis of one hundred patients. J Pediatr Orthop 1993;13:232-8. [Google Scholar]
- 3.Steinberg EL, Golomb D, Salama R, Wientroub S. Radial head and neck fractures in children. J Pediatr Orthop 1988;8:35-40. [Google Scholar]
- 4.Jeffery CC. Fractures of the head of the radius in children. J Bone Joint Surg Br 1950;32:314-24. [Google Scholar]
- 5.Newman JH. Displaced radial neck fractures in children. Injury 1977;9:114-21. [Google Scholar]
- 6.Chotel F, Vallese P, Parot R, Laville JM, Hodgkinson I, Muller C, et al. Complete dislocation of the radial head following fracture of the radial neck in children: The Jeffery Type II lesion. J Pediatr Orthop B 2004;13:268-74. [Google Scholar]
- 7.Navali AM, Sadigi A. Displaced fracture of the neck of the radius with complete 180 degrees rotation of the radial head during closed reduction. J Hand Surg Br 2006;31:689-91. [Google Scholar]
- 8.Wood SK. Reversal of the radial head during reduction of fracture of the neck of the radius in children. J Bone Joint Surg Br 1969;51:707-10. [Google Scholar]
- 9.Jeffery CC. Fractures of the neck of the radius in children. Mechanism of causation. J Bone Joint Surg Br 1972;54:717-9. [Google Scholar]
- 10.Kherbeck T, Gillani S, Ali AM. Reversed reduction of radial neck fractures; A predictable complication of closed manipulation. Inj Extra 2006;37:116-9. [Google Scholar]
- 11.Wray CC, Harper WM. The upside-down radial head: Brief report. Injury 1989;20:241-2. [Google Scholar]
- 12.Evans MC, Graham HK. Radial neck fractures in children: A management algorithm. J Pediatr Orthop B 1999;8:93-9. [Google Scholar]
- 13.Metaizeau JP, Lascombes P, Lemelle JL, Finlayson D, Prevot J. Reduction and fixation of displaced radial neck fractures by closed intramedullary pinning. J Pediatr Orthop 1993;13:355-60. [Google Scholar]
- 14.Chotel F, Sailhan F, Martin JN, Filipe G, Pem R, Garnier E, et al. A specific closed percutaneous technique for reduction of Jeffery Type II lesion. J Pediatr Orthop B 2006;15:376-8. [Google Scholar]
- 15.Shtarker H, Stahl S, Ross A, Bialik V. The ’upside-down’ radial head: A diagnostic challenge. J Pediatr Orthop B 2001;10:331-3. [Google Scholar]






