
Utilize the patellar fracture to asses and fix the distal femoral fractures before recreating the extensor mechanism to preserve soft-tissue attachments and blood supply to the patella.
Dr. Rutvik Dave, Department of Orthopaedics, Dr. M.K. Shah Medical College and Research Centre, Ahmedabad, Gujarat, India. E-mail: rutvikdave@gmail.com
Introduction: Open vertical patella fractures in combination with distal femoral or proximal tibial fractures are a rare combination of injuries that pose a challenge for adequate fixation and gaining favorable outcome.
Case Report: Case 1 had an open fracture of sagittal fracture of patella with one half comminuted and a sagittal plane fracture of lateral femoral condyle with a 2 × 2 cm of articular bone loss. Case 2 had an open sagittal fracture of patella with ipsilateral lateral femoral condyle fracture and proximal tibia medial condyle fracture in sagittal plane. Case 3 had a closed comminuted fracture of patella with sagittal plane lateral femoral condyle fracture.
Conclusion: Open vertical plane patella fractures with associated distal femoral or proximal tibial fracture when treated properly can restore knee function optimally.
Keywords: Vertical patella fracture, open knee injuries, complex knee trauma.
High-energy mechanisms of injury are increasing with increasing use of automobiles and it often leads to multiply fractured bones in a single joint due to overlapping force vectors at time of injury. Knee joint is one of the most frequently involved joints in such injuries. Bostrom in a series of 422 patients found an incidence of about 28% of vertical fracture of patella and a 6% incidence of open patella fractures overall. The combination of open vertical patella fracture is even rarer [1]. Open patella fractures are sometimes associated with fractures of distal femur, proximal tibia, hip dislocations, or acetabular fractures which make management of these injuries challenging [2, 3]. Here, we present three such rare cases of open vertical plane patella fractures with associated distal femoral or proximal tibial fracture that presented to our emergency room. Details regarding the initial treatment, mechanism of injury, grading of open fracture, surgery, and complications were taken from patient notes and were confirmed from the patients. Consent was obtained from each of these patients for the use of their data for publication purposes.
Case 1
A 40-year-male sustained an open Grade 3 vertical fracture of the right patella which was partially comminuted with an ipsilateral lateral femoral condyle fracture. It was a farmyard injury with penetration of metallic hook of a tractor with bone loss at place of injury discarded by the patient. There was no neurovascular deficit. The patient underwent emergency surgery after anesthesia clearance. The open wound was extended as needed for exploration and fixation. Intraoperatively, it was found that half of the patella was missing, the remaining half had few soft-tissue attachments and there was a defect in the articular surface of the lateral femoral condyle as shown in the image. As the patella was not salvageable, it was decided intraoperatively to do a patellectomy and use it as a bone graft to recreate articular surface of the femoral condyle. The lateral femoral condyle was reduced and fixed using cancellous screws and bone grafted patella was reshaped and positioned in the defect such that articular cartilage faces outward and held in place using K-wires which were left buried in situ. Tendon ends were repaired using non-absorbable sutures and patient was immobilized in a knee brace for 6 weeks. Static quadriceps was started from 1st post-operative day. Knee range of motion was started at 6 weeks. Partial weight-bearing started at 1.5 months and full weight-bearing at 2.5 months. The patient was advised to wear a removable knee brace while walking. At review 1 year after the injury, the patient had 100° of knee flexion with a 10° extension lag, was independently ambulatory, and complained of occasional pain and instability (Fig. 1a-d).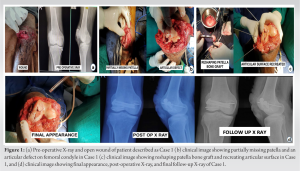
Case 2
A 33-year-female sustained an open Grade 2 vertical fracture of patella with a fracture of medial tibial condyle and lateral femoral condyle. She suffered a collision with a streetlight pole while seated in an autorickshaw with her leg out of the vehicle. She was taken for emergency surgical intervention after anesthetic clearance. She had a 5 cm wound on anterior aspect of knee which was extended proximally and distally to debride the wound and reduce and fix fracture fragments. The femur and tibial fractures were accessed through the fractured patella. First, the femoral condyle was fixed with 6.5 mm cannulated cancellous screws, followed by fixation of the tibial condyle with 6.5 mm cannulated cancellous screws, and lastly, the patella was fixed with screws. Limb was immobilized with a knee brace for 4 weeks. The patient was allowed movement at 4 weeks. Partial weight-bearing started at 2 months and full weight-bearing at 3.5 months. At review 1 year after the injury, the patient had 125° of knee flexion with no signs of patellofemoral or tibiofemoral arthritis and was symptom-free (Fig. 2a and b).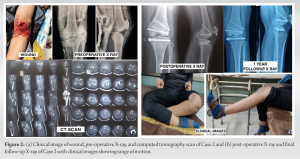
Case 3
A 30-year-male sustained an open Grade 2 comminuted fracture of the right patella with an ipsilateral lateral femoral condyle sagittal plane fracture. He suffered a road traffic accident with a direct impact to front of knee. The patient had no neurovascular deficit and was taken for emergency surgery after anesthetic clearance. Wound was extended proximally and distally, debridement was done and the comminuted patella was fixed first. Lateral parapatellar approach was taken in deeper plane and the patella was flipped to achieve anatomical articular alignment and fixed with cancellous screws and encirclage. Next, the lateral femoral condyle was addressed through same approach and reduced and fixed with screws and buttressed with a reconstruction plate. Limb was immobilized in a knee brace for 4 weeks after which passive mobilization started. Partial weight-bearing was allowed at 2 months while full weight-bearing allowed at 3 months. At review 1 year after surgery, the patient had 135° of knee flexion with no extension lag and was symptom-free (Fig. 3a and b).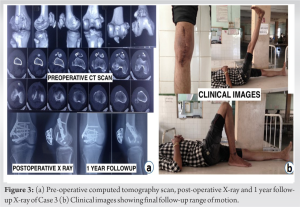
Patella fractures account for about 1% of all skeletal injuries [1]. Despite its subcutaneous location, open injuries of patella are rare. A vertical patella fracture is often of the lateral third of patella due to diminished resistance of lateral third since it has exclusively cancellous bone [4]. A combination of vertical patella fracture with a distal femoral or proximal tibia fracture is quite rare and is almost always due to a high-energy direct injury to the knee. We found only few case reports in the literature reporting the same. In the presence of multiple fractures in the same extremity, internal fixation of one or more of the fractures will greatly facilitate early joint mobilization and rehabilitation [5]. The management principles of such an injury are the same as that for any open injury which includes urgent debridement and stable fixation with preserving soft-tissue attachments. It is also important to recreate the extensor mechanism. Anterior knee pain is due to poor function of extensor mechanism as pain is often reported when the extensor mechanism is activated while the knee is under load in flexion. An atrophic and weak quadriceps leads to a maltracking patella and increased articular stress resulting in anterior knee pain that in turn inhibits muscle activity eventually leading to poorer outcomes [6]. Patella acts as a 3D lever around the patellofemoral contact area and the varying location of patella is the primary determinant of force ratios [7]. Hence, in open fractures of the patella, all attempts for preservation of bone substance and precise reconstruction of the extensors should be attempted, reserving total patellectomy as a salvage procedure [8]. Torchia and Lewallen reported a series of open patella fractures comprising of 14.5% type 1 injuries, 76.4% type 2 injuries, and 9.1% type 3 injuries as per Gustillo Anderson classification. Out of three of our cases, two are Grade 2 injuries and one is a Grade 3 injury. Anand et al. [9] reported a series of 20 open patella fractures which were all primarily fixed with no patellectomy performed primarily. In our cases, one patient had to undergo primary patellectomy. When addressing multiple injuries of knee joint, the issue of skin necrosis occurs due to close proximity of skin incisions. Lee et al. [10] reported the use of midline approach through the patellar fracture to address distal femoral fractures to avoid the same issue. In all our cases, we extended the midline incision and addressed the femoral or tibial injuries through same approach. In our first case, due to comminuted nature of patellar fracture and bone loss, patellectomy was performed and articular surface recreated. The patient had an unsatisfactory outcome due to inadequate extensor mechanism as well as nature of injury. Due to high-energy transferred, a greater degree of damage to soft-tissues, cartilage, and comminution is reported in such fractures by Torchia and Lewallen. Open patellar fractures have a higher rate of complications [1, 2]. To the best of our knowledge, no other such description of using patellar articular surface to recreate femoral articular surface has been reported. Patient 2 had a floating knee injury associated with a vertical patella fracture. Ran et al. [11] proposed a modified Fraser classification for floating knee injury according to which type 3 includes patella fracture not included in Fraser classification. Anatomical reduction of all three fractures was essential to restore knee function. Patient 3 had a comminuted patella fracture; however, effort was made to salvage patella with strategic compression screws to provided good extensor mechanism and allow early mobilization. One-year follow-up of these patients reported favorable outcomes. This however does not exclude a long-term potential for post-traumatic osteoarthritis. The authors intend to keep the patients in long-term follow-up to identify delayed arthritis.
Early surgery and early mobilization improves prognosis. In multiply injured patients, small functional limitations are justified by the higher-energy injury mechanism and exposure of fracture cartilage in open injuries. Anatomical reduction is necessary with a stable fixation to encourage early rehabilitation. Soft-tissues must be respected to improve rate of union and outcomes. Patellectomy must be resorted to only as salvage option. Sometimes thinking outside the box may lead to better outcomes for the patient.
Restoration of extensor mechanism is mandatory to achieve better functional outcome. Utilizing the fracture pattern to access associated fractures prevents loss of soft-tissue attachments and enables better fixation as well as earlier mobilization with favorable outcomes as highlighted in this case report.
References
- 1.Boström A. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl 1972;143:1-80. [Google Scholar]
- 2.Torchia ME, Lewallen DG. Open fractures of the patella. J Orthop Trauma 1996;10:403-9. [Google Scholar]
- 3.Larangeira JA, Bellenzier L, da Sliva Rigo V, Neto EJ, Krum FF, Ribeiro TA. Vertical open patella fracture, treatment, rehabilitation and the moment to fixation. J Clin Med Res 2015;7:129-33. [Google Scholar]
- 4.Black J, Conners J. Vertical fractures of the patella. South Med J 1969;62:76-7. [Google Scholar]
- 5.Hayes JT. Multiple fractures in the same extremity: Some problems in their management. Surg Clin North Am 1961;41:1379-88. [Google Scholar]
- 6.Lazaro LE, Wellman DS, Sauro G, Pardee NC, Berkes MB, Little MT, et al. Outcomes after operative fixation of complete articular patellar fractures: Assessment of functional impairment. J Bone Joint Surg Am 2013;95:e96 1-8. [Google Scholar]
- 7.Huberti HH, Hayes WC, Stone JL, Shybut GT. Force ratios in the quadriceps tendon and ligamentum patellae. J Orthop Res 1984;2:49-54. [Google Scholar]
- 8.Catalano JB, Iannacone WM, Marczyk S, Dalsey RM, Deutsch LS, Born CT, et al. Open fractures of the patella: Long-term functional outcome. J Trauma 1995;39:439-44. [Google Scholar]
- 9.Anand S, Hahnel JC, Giannoudis PV. Open patellar fractures: High energy injuries with a poor outcome? Injury 2008;39:480-4. [Google Scholar]
- 10.Lee SH, Kim MB, Sim JA, Han DH. A transpatellar approach to treat distal femoral Type C3 fractures combined with patellar fractures. J Knee Surg 2018;31:905-12. [Google Scholar]
- 11.Ran T, Hua X, Zhenyu Z, Yue L, Youhua W, Yi C, Fan L. Floating knee: A modified Fraser’s classification and the results of a series of 28 cases. Injury 2013;44:1033-42. [Google Scholar]





