
Complex traumas such as Neglected Monteggia fractures can be treated with a single incision surgery along with deep fascial ALR reconstruction with excellent results and outcomes.
Dr. Himansu Bhusan Behera, Department of Orthopaedics, Siksha O Anusandhan (Deemed to be University), Bhubaneswar, Odisha, India. E-mail: himansubehera71@gmail.com
Introduction: Chronic radial head dislocation in old standing or neglected Monteggia fracture is a devastating complication. We present our case regarding managing such a case using plating and fascial slip annular ligament reconstruction (ALR).
Case Report: A 40-year-old male patient, farmer by profession presented with a 4-month-old neglected Monteggia fracture. He was treated with open reduction and internal fixation of fracture ulna with ALR using forearm deep fascial slip. The patient underwent regular physiotherapy post-operatively after 2 weeks of surgery. The patient was followed for 6 months, and DASH score was used to evaluate functional outcome.
Conclusion: Excellent results were obtained as regards to pain, wrist range of motion, fracture union, and resuming routine activities at the follow-ups.
Keywords: Monteggia, fracture, annular ligament reconstruction.
Neglected Monteggia fractures are fractures of the proximal ulna with the dislocation of the radial head presenting after 4 weeks of the injury [1]. These chronic conditions are often associated with devastating complications such as ulnar displacement, malunion, or disruption leading to angulation and shortening of affected arm [2] as the radius follows the lower fragment due to the pull of the interosseous membranes [3]. The proximal radius and ulna along with the interosseous membrane and the annular ligament have a closed ring-like anatomy that predisposes to this condition. It is crucial to note that, unless proven otherwise by radiological or clinical survey, a single bone fracture of the forearm is to be treated as fracture dislocation, more often than not requiring surgical management. Various alternatives exist such as open or closed reduction of the radial head, transarticular fixation, ulnar or radial osteotomies, repair or reconstruction of the annular ligament, or some amalgamation of these techniques. Here, we present a case of a 4-month-old Monteggia fracture dislocation treated with annular ligament reconstruction (ALR) using forearm fascia which is a rare and less described procedure.
The Patient is a 40-years-old male farmer presented to our OPD with complaints of pain and deformity over RT elbow joint. He had a history of injury to right forearm due to fall from height with outstretched hand 4 month back, for which he received treatment from a local bone setter. He was not a known case of DM or HTN. Clinically, he had a varus deformity in his right elbow with restricted pronation and supination of the elbow. There was a palpable bony swelling over the lateral aspect just distal to elbow joint which tended to move upon forceful pronation and supination. The flexion and extension were up to full extent. There was no distal NVD. On measurement, right forearm was 2 cm shortened. He also had severe pain over the DRUJ. AP and lateral X-ray revealed a BADO Type 2 Monteggia fracture dislocation with the delayed union of ulna and anteriorly dislocated radial head (Fig. 1 and 2). 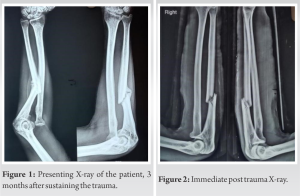 The fracture was approached through extended BOYD’S approach. The deep fascia of the fore arm was identified. A strip of fascia around 14 cm in length and 1 cm in breadth was harvested carefully using a 15 mm BP blade with intact base over the olecranon (Fig. 3). Joint was approached through ECU and anconeus muscle. The annular ligament was found to be completely disrupted. The radial head was carefully delivered. The soft tissues attached with the head and neck part were kept intact for ALR.
The fracture was approached through extended BOYD’S approach. The deep fascia of the fore arm was identified. A strip of fascia around 14 cm in length and 1 cm in breadth was harvested carefully using a 15 mm BP blade with intact base over the olecranon (Fig. 3). Joint was approached through ECU and anconeus muscle. The annular ligament was found to be completely disrupted. The radial head was carefully delivered. The soft tissues attached with the head and neck part were kept intact for ALR. 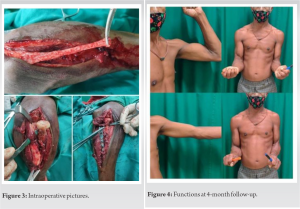 Radial groove of ulna and capitulum was cleared. Radial head was relocated, and congruency was confirmed. Next, the fracture site was cleared and refreshened. The fracture ends were assembled and fixed with a 7-hole LCDCP after putting bone grafts at the fracture sites from ipsilateral iliac bone. After fixation of the bone and length restoration, the fascial sling was bound over the radial neck region keeping adequate tension and re-enforced with 3–0 proline (Fig. 3). An additional transcapitular k-wire was applied at 90° elbow flexion. Wound was closed in layered over 12-size Romo Vac drain. Sterile dressing and above-elbow slab were given. After 1 month, slab and k-wire was removed, and gradual mobilization was started. The full extension and flexion, around 75° of external and internal rotation was restored within 2 months of gradual supervised physiotherapy (Fig. 4). Good bony union was achieved (Fig. 5 and 6), and the patient is now able to do all his daily living activities. The DASH score has improved to 56 and we are hopeful for gradual recovery and full restoration of movements with aggressive physiotherapy within the next 2–3 months. Regular follow-up was kept of the patient. At the end of 1 year, his DASH score improved to 74 with complete radiological union of the fractures (Fig. 7). He is currently able to perform his daily activities and livelihood without much difficulty.
Radial groove of ulna and capitulum was cleared. Radial head was relocated, and congruency was confirmed. Next, the fracture site was cleared and refreshened. The fracture ends were assembled and fixed with a 7-hole LCDCP after putting bone grafts at the fracture sites from ipsilateral iliac bone. After fixation of the bone and length restoration, the fascial sling was bound over the radial neck region keeping adequate tension and re-enforced with 3–0 proline (Fig. 3). An additional transcapitular k-wire was applied at 90° elbow flexion. Wound was closed in layered over 12-size Romo Vac drain. Sterile dressing and above-elbow slab were given. After 1 month, slab and k-wire was removed, and gradual mobilization was started. The full extension and flexion, around 75° of external and internal rotation was restored within 2 months of gradual supervised physiotherapy (Fig. 4). Good bony union was achieved (Fig. 5 and 6), and the patient is now able to do all his daily living activities. The DASH score has improved to 56 and we are hopeful for gradual recovery and full restoration of movements with aggressive physiotherapy within the next 2–3 months. Regular follow-up was kept of the patient. At the end of 1 year, his DASH score improved to 74 with complete radiological union of the fractures (Fig. 7). He is currently able to perform his daily activities and livelihood without much difficulty.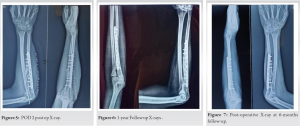
Giovanni Battista Monteggia In 1814, in his paper printed in Instituzioni Chirurgiches, first narrated an injury distinguished by the anterior dislocation of the radial head associated with ulnar diaphyseal fractures [5]. The complexity of this injury was not to be fully appreciated until it was coined in English as “Monteggia lesion” by Bado [6]. Subsequently, it has been realized that Monteggia fracture dislocations are complex injuries, accounting for nearly 13% of all forearm fractures [6]. Dislocation of the radial head that is still present 4 weeks after injury is recognized as chronic Monteggia fracture. Such a circumstance may lead to decreased range of motion associated elbow affliction, neurologic deficits, and valgus deformity [7, 8, 9]. In such a scenario, in order for the proximal radioulnar joint to be reduced, rigid anatomic reduction, and fixation of the ulnar diaphyseal fracture is advocated. It is also essential to maintain <10° angulation to ensure optimal proximal radioulnar joint stability and functionality. Nevertheless, complex Monteggia fracture–dislocations even after proper surgical treatment may be riddled with have a high rate of low clinical outcomes associated with numerous complications [12, 13, 14]. A probable cause can be due to either the residual ulnar deformity even after internal fixation (secondary to non-union or non-anatomic reduction) or the failure of spontaneous healing of the annular ligament. In 1965 Tawse et al., in their paper narrated a technique where using the triceps tendon, the annular ligament was reconstructed [15]. The authors had proposed that any interposed capsule if any should be first removed before anatomic reduction of the radial head. Following this, the tendon strip that was left attached to the ulna was brought forward from the posterior to the anterior side, made to go around the radial head before being fixed to the proximal ulna with the help of a drill hole. Such similar ALR techniques using triceps tendon were also described by other authors [16, 17]. Lloyd-Roberts and Bucknill suggested a modification to the original Tawse technique where ALR was done using lateral part of the triceps tendon bundle [17]. Steel and Peterson suggested using interference screws instead for ligament reconstruction or repair using triceps tendon at the level of the origin of the annular ligament [18]. Some authors even have proposed using the superficial head of the Brachialis muscle ALR [19, 20]. Using fascial sling for ALR is a relatively new technique and has not been very well described in literatures. When compared with Tawse and other described techniques of ALR, this method requires single incision for both fracture fixation and graft harvesting. Obviously, it has easier learning curve, less donor side morbidity, and shorter operative time. Furthermore, early mobilization and physiotherapy can be allowed which leads to early functional recovery and return to work.
It is absolutely crucial to achieve bony alignment of the ulna to effectively manage chronic Monteggia fractures. However, ALR is critical for stability of radial head in these neglected injuries. Forearm fascia is a novel and ideal graft to be used as sling around radial neck. In good hands, excellent results are expected. However, further studies on more number of patients are required in this regard.
Owing to the poor clinical outcomes in neglected Monteggia fractures, the use of triceps tendon for ALR was suggested by Tawse, modified later by Llyod-Roberts and Bucknill where only the lateral part of the tendon was used. Using deep fascia instead is a newer and novel technique not much explored. Advantages include single incision, less donor side morbidity, and shorter operative time. Bony alignment of Ulna and ALR is crucial for the stability of the radial head, elbow joint, and eventually favorable clinical outcomes.
References
- 1.Goh SH. Monteggia ‘fracture’-dislocation with bowing of the ulna: A pitfall for the unwary emergency physician. Eur J Emerg Med 2008;15:281-2. [Google Scholar]
- 2.Nakamura K, Hirachi K, Uchiyama S, Takahara M, Minami A, Imaeda T, et al. Long-Term clinical and radiographic outcomes after open reduction for missed monteggia fracture-dislocations in children. J Bone Joint Surg Am 2009;91:1394-404. [Google Scholar]
- 3.Cunnighan SR. Fracture of ulna with dislocation of head of radius. J Bone Joint Surg Am 1934;16:351-4. [Google Scholar]
- 4.Korner J, Hansen M, Weinberg A, Hessmann M, Rommens PM. Monteggia fractures in childhood diagnosis and management in acute and chronic cases. Eur J Trauma 2004;30:361-70. [Google Scholar]
- 5.Beaty JH, Kasser JR. Monteggia fracture-dislocation in children. In: Rockwood and Wilkins’ Fractures in Children. 6th ed. Riverwoods, IL: Lippincott Williams and Wilkins; 2006. p. 447-551. [Google Scholar]
- 6.Bado JL. The monteggia lesion. Springfield, IL: Charles C Thomas; 1962. [Google Scholar]
- 7.Olney BW, Menelaus MB. Monteggia and equivalent lesions in childhood. J Pediatr Orthop 1989;9:219-23. [Google Scholar]
- 8.Peiró A, Andres F, Fernandez-Esteve F. Acute monteggia lesions in children. J Bone Joint Surg Am 1977;59:92-7. [Google Scholar]
- 9.Reckling FW. Unstable fracture-dislocations of the forearm: Monteggia and galeazzi lesions. J Bone Joint Surg Am 1982;64:857-63. [Google Scholar]
- 10.Dormans JP, Rang M. The problem of monteggia fracture-dislocations in children. Orthop Clin North Am 1990;21:251-6. [Google Scholar]
- 11.Letts M, Locht R, Wiens J. Monteggia fracture-dislocations in children. J Bone Joint Surg Br 1985;67:724-7. [Google Scholar]
- 12.Wiley JJ, Galey JP. Monteggia injuries in children. J Bone Joint Surg Br 1985;67:728-31. [Google Scholar]
- 13.Bryan RS. Monteggia fracture of the forearm. J Trauma 1971;11:992-8. [Google Scholar]
- 14.Fowles JV, Sliman N, Kassab MT. The monteggia lesion in children. Fracture of the ulna and dislocation of the radial head. J Bone Joint Surg Am 1983;65:1276-82. [Google Scholar]
- 15.Tawse AB. The treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Am 1965;47:718-23. [Google Scholar]
- 16.Boyd HB, Boals JC. The Monteggia lesion: A review of 159 cases. Clin Orthop Relat Res 1969;66:94-100. [Google Scholar]
- 17.Lloyd-Roberts GC, Bucknill TM. Anterior dislocation of the radial head in children: Etiology, natural history and management. J Bone Joint Surg Br 1977;59:402-7. [Google Scholar]
- 18.Seel MJ, Peterson HA. Management of chronic posttraumatic radial head dislocation in children. J Pediatr Orthop 1999;19:306-12. [Google Scholar]
- 19.Leonello DT, Galley IJ, Bain GI, Carter CD. Brachialis muscle anatomy: A study in cadavers. J Bone Joint Surg Am 2007;89:1293-7. [Google Scholar]
- 20.Nwoko OE, Patel PP, Richard MJ, Leversedge FJ. Annular ligament reconstruction using the distal tendon of the superficial head of the brachialis muscle: An anatomical feasibility study. J Hand Surg Am 2013;38:1315-9. [Google Scholar]






