
Transposition osteotomy of the acetabulum can be effective for subchondral fracture of the femoral head with acetabular dysplasia.
Dr. Yoshiaki Miyake, Department of Bone and Joint Surgery, Kawasaki Medical School, Matsushima, Kurashiki, Japan. E-mail: miyakeyoshiakimiyake@yahoo.co.jp
Introduction: Subchondral insufficiency fracture of the femoral head commonly occurs in older women with osteoporosis. However, subchondral fatigue fracture of the subchondral femoral head is rare. We present a rare case of fatigue fracture of the subchondral femoral head with acetabular dysplasia.
Case Report: The patient was a 16-year-old male, height 180 cm, weight 112 kg, and body mass index 34.6 kg/m2. Continuous right hip pain appeared after club activity of table tennis a month before admission to our department. Pain was observed on deep flexion of the right hip joint. The FADIR test was positive. X-ray images showed a depressed deformity of the right femoral head loading area. In addition, the center-edge angle was 10° on the right and 21° on the left, tear drop distance was 12 mm on the right and 8 mm on the left, and bilateral acetabular dysplasia was noted. In magnetic resonance imaging, the T1-weighted image shows low-intensity signal and the T2-weighted image shows high-intensity signal, indicating a fatigue fracture of the femoral head with subchondral depression. Thus, transposition osteotomy of the acetabulum was performed in this case. Postoperatively, the depression portion showed gradual remodeling, and the patient returned to sports after 6 months. Because this patient was highly obese with acetabular dysplasia, a large shear force was applied to the loading portion of the femoral head relative to the acetabular rim. The femoral head was repeatedly forced, resulting in a fatigue fracture. We believe that the stress applied to the depressed portion was dispersed by the transposition osteotomy of the acetabulum, resulting in remodeling.
Conclusion: This is the first report of the transposition osteotomy of the acetabulum for a subchondral fatigue fracture of the femoral head with acetabular dysplasia. Thus, this may serve as a reference in the management of such rare occurrences and pave the way for further understanding of this condition.
Keywords: Femoral head fracture, acetabular dysplasia, transposition osteotomy of the acetabulum
Stress fractures are caused by repetitive forces and are classified into three categories: fatigue fracture, insufficiency fracture, and pathological fracture [1]. Fatigue fractures are caused by non-physiological stress, such as sports action on a bone of normal strength. Insufficiency fractures are caused by physiological external forces of daily living acts on bones with reduced strength, such as in cases of osteoporosis. Bangil proposed the concept of subchondral insufficiency fracture of the femoral head in 1996 [2]. It commonly occurs in older women with osteoporosis (average 68–72 years of age) [3, 4], and results in osteoarthritis [5]. Conversely, subchondral fatigue fractures of the femoral head in young people have also been reported, although they are rare [6, 7]. In this study, along with a literature review, we report a case of subchondral fatigue fracture of the femoral head in a high school student with acetabular dysplasia.
The patient was a 16-year-old male high school freshman. He was 180 cm tall, weighed 112 kg, and was obese, with body mass index of 34.6 kg/m2. He had no history of treatment or family history of hip disease, including developmental hip dysplasia. He had no other notable underlying medical conditions. One month ago, right hip joint pain appeared after table tennis club activity, and the pain did not improve, for which he presented to our department. The range of passive motion of the hip joint was as follows: right flexion, 80°; left flexion, 100°; right abduction, 30°; left abduction, 30°; right adduction, 10°; left adduction, 10°; right internal rotation, 0°; left internal rotation, 10°; right external rotation, 40°; and left external rotation, 40°. The patient had pain on deep flexion of the right hip joint, a negative FABER test, and a positive FADIR test. X-ray images showed a depressed deformity of the right femoral head loading portion. The center-edge angle (CE angle) was 10° on the right and 21° on the left, and the teardrop distance was 12 mm on the right and 8 mm on the left; he had bilateral acetabular dysplasia (Fig. 1). Computed tomography (CT) images showed a depression at the load-bearing portion of the femoral head opposite to the acetabular rim (Fig. 2). Magnetic resonance imaging showed low-intensity signal on T1-weighted images and high-intensity signal on T2-weighted images (Fig. 3), for which a subchondral fatigue fracture with femoral head depression was diagnosed. Transposition osteotomy of the acetabulum was performed in this case. 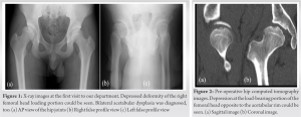 In the left lower lateral recumbent position, a U-shaped skin incision was developed on the lateral side of the hip joint. The greater trochanter was detached and translated to approach the external plate of the iliac crest. After the pubic osteotomy, the iliac bone was osteotomized to the internal plate and the bone fragment was rotated anterolaterally. Intraoperative fluoroscopic images showed leveling of the loading portion and medialization of the femoral head. The mobile fragment was fixed with two 6.5 mm-diameter poly-L-lactic acid screws.
In the left lower lateral recumbent position, a U-shaped skin incision was developed on the lateral side of the hip joint. The greater trochanter was detached and translated to approach the external plate of the iliac crest. After the pubic osteotomy, the iliac bone was osteotomized to the internal plate and the bone fragment was rotated anterolaterally. Intraoperative fluoroscopic images showed leveling of the loading portion and medialization of the femoral head. The mobile fragment was fixed with two 6.5 mm-diameter poly-L-lactic acid screws. 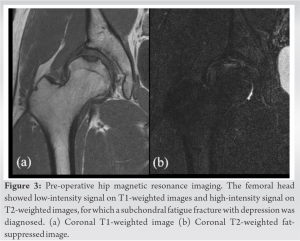 The detached greater trochanter was fixed with two 6.5 mm-diameter titanium screws. Post-operative X-ray image (Fig. 4) showed a CE angle of 30° and improved hip coverage. After 5 weeks of non-weight-bearing on the right lower extremity, one-third partial weight-bearing was permitted, half partial weight-bearing after 7 weeks, and full weight-bearing at 9 weeks postoperatively. The depressed portion of the femoral head showed gradual remodeling, and the patient returned to sports 6 months after surgery. Two years after surgery, CT images before removal of the titanium screw showed that the depressed portion of the femoral head had almost completely remodeled (Fig. 5). At the last observation 2 years and 5 months after surgery, X-ray image showed no osteoarthritis (Fig. 6). There was no pain or limitation of range of motion in the right hip joint, which did not interfere with daily life or sports.
The detached greater trochanter was fixed with two 6.5 mm-diameter titanium screws. Post-operative X-ray image (Fig. 4) showed a CE angle of 30° and improved hip coverage. After 5 weeks of non-weight-bearing on the right lower extremity, one-third partial weight-bearing was permitted, half partial weight-bearing after 7 weeks, and full weight-bearing at 9 weeks postoperatively. The depressed portion of the femoral head showed gradual remodeling, and the patient returned to sports 6 months after surgery. Two years after surgery, CT images before removal of the titanium screw showed that the depressed portion of the femoral head had almost completely remodeled (Fig. 5). At the last observation 2 years and 5 months after surgery, X-ray image showed no osteoarthritis (Fig. 6). There was no pain or limitation of range of motion in the right hip joint, which did not interfere with daily life or sports.
If femoral head fractures occur at the loading portion, they are likely to progress to osteoarthritis. For this reason, early detection and appropriate treatment is necessary [8]. Femoral head fractures in young people are commonly associated with hip dislocation [9, 10], although some without dislocation have been reported [11, 12, 13]. However, subchondral fatigue fracture of the femoral head is very rare and most reports involve military personnel and top athletes [6, 7]. Although the present case was a table tennis player at the high school club level, subchondral fatigue fracture of the femoral head occurred. In recent years, dysplasia has been discussed as a cause of subchondral fractures of the femoral head in the elderly [14, 15]. However, it has been reported that retroversion, not dysplasia, is related to subchondral fractures of the femoral head in young people [16]. This patient had acetabular dysplasia rather than acetabular retroversion. To our knowledge, there are no reports of subchondral fatigue fracture of the femoral head with acetabular dysplasia in young people. In acetabular dysplasia, it is considered that the stress applied to the load-bearing portion increases according to its severity [17]. In addition, in recent years, the concept of inside-out lesion has been proposed for cartilage and labrum injury with acetabular dysplasia [18]. In this case, it is considered that large shear stress was repeatedly applied to the femoral head-loaded portion opposite to the acetabular rim due to acetabular dysplasia with a CE angle of 10° and a high body weight of 100 kg or more, resulting in fatigue fracture. Kim et al. reported on 34 cases of subchondral fatigue fracture of the femoral head in young patients, 12 of which had a loss of sphericity of the femoral head due to a collapse of the articular margin, requiring hip replacement surgery [19]. In this case, the sphericity of the femoral head was also lost at the time of initial visit to our department, and poor prognosis was predicted. However, there is a Japanese report where a transtrochanteric rotational osteotomy was performed for a subchondral fracture of the femoral head that had already depressed and showed good results [20]. Transtrochanteric rotational osteotomy was originally a surgery aimed at reducing hip symptoms of femoral head necrosis by moving the necrotic portion to the non-loading surface and the healthy portion to the loading surface. In the aforementioned report, good results were obtained by remodeling, moving the subchondral fractured portion of the femoral head to the non-loading surface. In this case, acetabular dysplasia was thought to be the cause of the subchondral fracture of the femoral head, so surgery was performed on the acetabulum side instead of the femoral side. Transposition osteotomy of the acetabulum improved the acetabular coverage, which distributed the stress on the fractured portion and resulted in remodeling.
This case report presents a 16-year-old male patient with a subchondral fatigue fracture of the femoral head with acetabular dysplasia. His condition was improved through the transposition osteotomy of the acetabulum. This is the first report of a transposition osteotomy of the acetabulum for a subchondral fatigue fracture of the femoral head with acetabular dysplasia. Thus, this may serve as a reference in the management of such rare occurrences and pave the way for further understanding of this condition.
Subchondral fatigue fracture of the femoral head with acetabular dysplasia is very rare. The transposition osteotomy of the acetabulum improved the acetabular coverage, which distributed the stress on the fractured portion and resulted in remodeling.
References
- 1.Pentecost RL, Murray RA, Brindley HH. Fatigue, insufficiency, and pathological fractures. JAMA 1964;187:1001-4. [Google Scholar]
- 2.Bangil M, Soubrier M, Dubost JJ, Rami S, Carcanagues Y, Ristori JM, et al. Subchondral insufficiency fracture of the femoral head. Rev Rhum Engl Ed 1996;63:859-61. [Google Scholar]
- 3.Yamamoto T, Bullough PG. The role of subchondral insufficiency fracture in the rapid destruction of the hip joint. Arthritis Rheum 2000;43:2423-7. [Google Scholar]
- 4.Chen M, Wang X, Takahashi E, Kaneuji A, Zhou Y, Kawahara N. Current research on subchondral insufficiency fracture of the femoral head. Clin Orthop Surg. 2022 Dec;14(4):477-485. doi: 10.4055/cios22175. Epub 2022 Nov 14. PMID: 36518923; PMCID: PMC9715932. [Google Scholar]
- 5.Shimizu T, Yokota S, Kimura Y, Asano T, Shimizu H, Ishizu H, Iwasaki N, Takahashi D. Predictors of cartilage degeneration in patients with subchondral insufficiency fracture of the femoral head: a retrospective study. Arthritis Res Ther. 2020 Jun 22;22(1):150. doi: 10.1186/s13075-020-02243-7. PMID: 32571393; PMCID: PMC7310243. [Google Scholar]
- 6.Visuri T. Stress osteopathy of the femoral head. 10 military recruits followed for 5-11 years. Acta Orthop Scand 1997;68:138-41. [Google Scholar]
- 7.Song WS, Yoo JJ, Koo KH, Yoon KS, Kim YM, Kim HJ. Subchondral fatigue fracture of the femoral head in military recruits. J Bone Joint Surg Am 2004;86:1917-24. [Google Scholar]
- 8.Delee JC, Evans JA, Thomas J. Anterior dislocation of the hip and associated femoral head fractures. J Bone Joint Surg 1980;62:960-4. [Google Scholar]
- 9.Pipkin G. Treatment OG grade IV fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39:1027. [Google Scholar]
- 10.Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop 1985;201:9-17. [Google Scholar]
- 11.Mody BS, Wainwright AM. Fracture of the femoral head without associated hip dislocation following low-energy trauma. Trauma Surg 1996;115:300-2. [Google Scholar]
- 12.Matsuda DK. A rare fracture, an even rarer treatment: The arthroscopic reduction and internal fixation of an isolated femoral head fracture. Arthroscopy 2009;25:408-12. [Google Scholar]
- 13.Yoon PW, Jeong HS, Yoo JJ, Hoo KH, Yoon KS, Kim HJ. Femoral head fracture without dislocation by low-energy trauma in a young adult. Clin Orthop Surg 2011;3:336-41. [Google Scholar]
- 14.Ishihara K, Miyanishi K, Ihara H, Jingushi S, Torisu T. Subchondral insufficiency fracture of the femoral head may be associated with hip dysplasia: a pilot study. Clin Orthop Relat Res. 2010 May;468(5):1331-1335. [Google Scholar]
- 15.Iwasaki K, Yamamoto T, Motomura G, Karasuyama K, Sonoda K, Kubo Y, Iwamoto Y. Common site of subchondral insufficiency fractures of the femoral head based on three-dimensional magnetic resonance imaging. Skeletal Radiol. 2016 Jan;45(1):105-113. [Google Scholar]
- 16.Kubo Y, Motomura G, Utsunomiya T, Fujii M, Ikemura S, Sonoda K, Nakashima Y. Distribution of femoral head subchondral fracture site relates to contact pressures, age, and acetabular structure. AJR Am J Roentgenol. 2020 Aug;215(2):448-457. [Google Scholar]
- 17.Pauwels F. Biomechanics of the normal and diseased hip. In: Theoretical Foundation, Technique and Results of Treatment. An Atlas. Germany: Sringer-Verlag; 1976. [Google Scholar]
- 18.Kraeutler MJ, Goodrich JA, Fioravanti MJ, Garabekyan T, Mei-Dan O. The “outside-in” lesion of hip impingement and the “inside-out” lesion of hip dysplasia: Two distinct patterns of acetabular chondral injury. Am J Sports Med 2019;47:2978-84. [Google Scholar]
- 19.Kim SM, Oh SM, Cho CH, Lim SJ, Moon YW, Choi SH, et al. Fate of subchondral fatigue fractures of the femoral head in young adults differs from the general outcome of fracture healing. Injury 2016;47:2789-94. [Google Scholar]
- 20.Yamamoto T, Iwasaki K, Iwamoto Y. Transtrochanteric rotational osteotomy for a subchondral insufficiency fracture of the femoral head in young. Clin Orthop Relat Res 2010;468:3181-5. [Google Scholar]




