
Gigantic musculoskeletal tumors are unusual, still limb salvage surgery is possible with experienced team, meticulous planning, and well-equipped treatment facility.
Dr. Raj Kumar Harshwal, Department of Orthopedics, SMS Medical College, Jaipur, Rajasthan, India. E-mail-drrajkharsh@gmail.com
Abstract
Introduction: Malignant transformation of pelvic osteochondroma is a rare entity. Large size and late presentation impose threat to life as well as limb. We report a case of limb salvage surgery in an enormously large secondary chondrosarcoma arising from pelvic bone.
Case Report: A 60-year-old male presented with a colossal swelling at groin reaching up to distal thigh. He was walking with a wide-based gait due to pain and discomfort. 30 year back, the patient first reported this swelling of pea size, for which he was advised surgery but due to fear of surgery and economic reason he refused. Swelling gradually increased in size and reached up to distal thigh in the past 30 years. It was hard and non-tender up to 6 months back, when suddenly a change in consistency from hard to soft in distal area was noticed. On examination, a large soft cystic swelling was hanging from his pubic area. Tumor was fixed at base on proximal end. On magnetic resonance imaging, size of tumor was 281 mm in length, 263 mm in width, and 250 mm in anteroposterior diameter. Tumor was arising from superior and ischiopubic rami. However, no intra-articular extension was seen. A radiographic skeletal survey and bone scan did not reveal any other lesion. On biopsy, chondrogenic tumor composed of lobules of chondroid material with no cellular atypia or evidence of malignancy was reported. Considering the age of patient, rapid progression in recent months, size and duration of tumor, and type 3 pelvic resection was planned. Using utilitarian pelvic incision with perineal extension, separating long adductor muscles and deep femoral artery tumor, tumor excised with osteotomy at pubic symphysis, and on superior and inferior pubic rami. With minor wound complications, wound healed in 3 weeks. Post-operative biopsy reported as Grade 1 chondrosarcoma. At 3-year follow–up, the patient has no complains and no sign of recurrence noticed.
Conclusion: Limb salvage surgery is a suitable option even in enormously large musculoskeletal malignancy. Proper counseling and tracking of patients are must to avoid future complications.
Keywords: Secondary pelvic chondrosarcoma, pelvic resection, limb saving surgery.
Osteochondromas are common, benign tumors known for their small size and slowly progressive nature. These commonly present over proximal tibia and humerus and distal femur, with rare sites being scapula, hand, foot, and pelvis [1,2]. Malignant transformation to secondary chondrosarcoma is seen in 0.5–5% of cases [3,4,5]. The case being presented by us is exceptional because of its long duration, huge size, and with malignant transformation yet successful limb salvage surgery was achieved.
A 60-year-old male patient came to orthopedics outpatient department with a huge swelling arising from groin and extending up to the left distal thigh. The patient complained of difficulty in walking and dragging sensation of lower abdomen. He was walking with a wide-based gait due to pain and discomfort. The patient initially noticed a small pea-sized swelling on his pubic area 30 years back, for which he was advised surgery at a local hospital, but he refused surgery due to fear and economic reasons. The swelling gradually progressed and reached up to distal thigh (Fig. 1).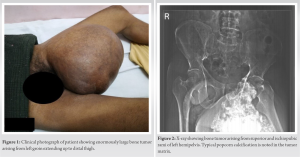 It was hard and non-tender up to 6 months back, when suddenly a change in consistency from hard to soft in distal area was noticed. He had an episode of fever and difficulty in micturition 2 months back, for which he took antibiotics and analgesics. On examination, a large soft cystic swelling was hanging from his pubic area. Penis and testicles were separate and deviated to left side, margins were not defined, and edge could not be felt on lateral side and pubic symphysis. The tumor was hard in consistency at its proximal area and soft on distal hanging area. Temperature was afebrile, no venous engorgement, and deep venous thrombosis was seen and translucency test was negative. Tumor was fixed to base on proximal end. On X-ray bone, tumor was arising from superior and ischiopubic rami of left hemipelvis. Typical popcorn calcification was noted in the tumor matrix (Fig. 2). On magnetic resonance imaging, lesion showed heterogeneous signals on T1 after intravenous contrast and hyperintense on T2-weighted images. Size of tumor was 281 mm in length, 263 mm in width, and 250 mm in anteroposterior diameter (Fig. 3).
It was hard and non-tender up to 6 months back, when suddenly a change in consistency from hard to soft in distal area was noticed. He had an episode of fever and difficulty in micturition 2 months back, for which he took antibiotics and analgesics. On examination, a large soft cystic swelling was hanging from his pubic area. Penis and testicles were separate and deviated to left side, margins were not defined, and edge could not be felt on lateral side and pubic symphysis. The tumor was hard in consistency at its proximal area and soft on distal hanging area. Temperature was afebrile, no venous engorgement, and deep venous thrombosis was seen and translucency test was negative. Tumor was fixed to base on proximal end. On X-ray bone, tumor was arising from superior and ischiopubic rami of left hemipelvis. Typical popcorn calcification was noted in the tumor matrix (Fig. 2). On magnetic resonance imaging, lesion showed heterogeneous signals on T1 after intravenous contrast and hyperintense on T2-weighted images. Size of tumor was 281 mm in length, 263 mm in width, and 250 mm in anteroposterior diameter (Fig. 3). Tumor was arising from superior pubic rami and ischiopubic rami and was reaching up to acetabular margins. However, no intra-articular extension was seen. A radiographic skeletal survey and bone scan did not reveal any other lesions. Computed tomography angiography was done to locate vessels and to identify tumor relationship to vessels (Fig. 4). Although the tumor was abutting to deep femoral artery, yet fat planes were maintained with common femoral, superficial, and deep femoral arteries. Needle biopsy showed chondrogenic tumor composed of lobules of chondroid material with only occasional chondrocytes. No cellular atypia or evidence of malignancy was seen. Considering the age of patient, rapid progression in recent months, size and duration of tumor, wide resection/and type 3 pelvic resection were planned. In supine position, illioinguinal component of utilitarian pelvic incision with perineal extension was used. Perineal extension was extended till distal extent of tumor. Lateral dissection was completed with the separation of long adductor muscles and deep femoral artery. Tumor was removed by doing osteotomy at pubic symphysis on superior and inferior pubic rami (Fig. 5).
Tumor was arising from superior pubic rami and ischiopubic rami and was reaching up to acetabular margins. However, no intra-articular extension was seen. A radiographic skeletal survey and bone scan did not reveal any other lesions. Computed tomography angiography was done to locate vessels and to identify tumor relationship to vessels (Fig. 4). Although the tumor was abutting to deep femoral artery, yet fat planes were maintained with common femoral, superficial, and deep femoral arteries. Needle biopsy showed chondrogenic tumor composed of lobules of chondroid material with only occasional chondrocytes. No cellular atypia or evidence of malignancy was seen. Considering the age of patient, rapid progression in recent months, size and duration of tumor, wide resection/and type 3 pelvic resection were planned. In supine position, illioinguinal component of utilitarian pelvic incision with perineal extension was used. Perineal extension was extended till distal extent of tumor. Lateral dissection was completed with the separation of long adductor muscles and deep femoral artery. Tumor was removed by doing osteotomy at pubic symphysis on superior and inferior pubic rami (Fig. 5).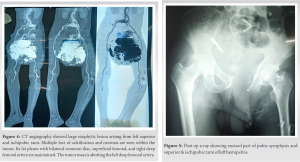 Due care was given to the urethra. The rest of the structures were repaired using polypropylene hermia mesh and non-absorbable ethibond 2 sutures. An urethrogram and bladder cystography was done post-operatively to rule out any leakage. Wound dehiscence was noticed on medial aspect which was treated with dressing and compression which was healed in 3 weeks (Fig. 6).
Due care was given to the urethra. The rest of the structures were repaired using polypropylene hermia mesh and non-absorbable ethibond 2 sutures. An urethrogram and bladder cystography was done post-operatively to rule out any leakage. Wound dehiscence was noticed on medial aspect which was treated with dressing and compression which was healed in 3 weeks (Fig. 6). 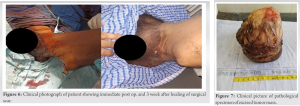 Post-operative biopsy revealed Grade 1 chondrosarcoma with clear margins (Fig. 7). Walking with support was allowed on 3rd post-operative day. Injectable antiobiotics (inj. cefuroxime 1.5 g bd) were given for three postoperative days thereafter oral for 3 weeks. The patient was followed up at 1, 3, and 6 months till 3 years. At final follow–up, final is asymptomatic with no signs of recurrence or metastasis.
Post-operative biopsy revealed Grade 1 chondrosarcoma with clear margins (Fig. 7). Walking with support was allowed on 3rd post-operative day. Injectable antiobiotics (inj. cefuroxime 1.5 g bd) were given for three postoperative days thereafter oral for 3 weeks. The patient was followed up at 1, 3, and 6 months till 3 years. At final follow–up, final is asymptomatic with no signs of recurrence or metastasis.
Osteochondromas are common, benign, usually asymptomatic tumors with >1/50000 incidences in the general population, though they account for 35% of benign and 8% of all bone tumors [1,2,3]. Generally presenting in the 2–3 decade of life, the incidence is grossly underestimated because of their asymptomatic nature. Treatment of osteochondromas is often ignored due its benign and indolent nature till it affects the esthetics or impinges on some important structure causing secondary sequelae or it starts undergoing malignant changes as it happened in our case [6,7]. Malignant transformation to a secondary chondrosarcoma is rare and serious complication seen in 0.3–5% of cases, especially in cases affecting the pelvic region [3,4,5]. An increase in size or change in consistency and of radiographic appearance should raise the suspicion of malignancy. Suspicious signs of malignancy on radiograph include surface irregularity, areas of lucency and heterogeneous mineralization, and thick cartilage cap (<2 cm) [8]. Surgery with wide margins is treatment of choice with 5-year survival rate reported from 70 to 80% for low-grade lesions and 40–50% for high-grade lesions. Metastases are rare in such cases, most common site being lungs. The prognosis is generally poor in case of these secondary metastases [9,10]. Our case is unique because of its exceptionally large dimensions (281 × 263 × 250 mm) and unique presentation. Despite the discomfort in walking and activities of daily living activities, with progression in size, the patient did not suffer any major sequeually and only deferred treatment for three decades because of fear and ignorance. Limb salvage surgery is an arduous task in such prodigious tumors. Difficulty in finding planes during surgery, surgery-related bleeding, reconstruction of large void of soft tissue after tumor resection, and post-surgery pelvic floor-related complications are associated with surgery of such colossal tumors. Meticulous planning, experienced anesthetist, blood bank support, and intensive care unit back up facility are paramount for attempting such surgeries. Despite its long-standing nature, the tumor remained benign and developed malignant changes in its distal part only in the past 6 months. No associated secondary metastases, lymph node involvement, or local invasion was seen making it a low-grade malignancy. No physical impairment and metastasis were noted on 3-year follow-up despite the large size of the malignancy. The largest tumor documented in Guinness World Record is 45 × 30 cm. size bone tumor removed from the right thigh of a 35–year-old male at Himalyan Institute of Medical Sciences, Dehradoon on March 10, 2002 [11]. To our knowledge, only two cases [11,12] of tumor excision, comparable to the present case, have been reported in literature. In both cases, limb had to be amputated for excision of tumor. Probably, this is the first case of giant secondary chondrosarcoma of pelvic origin, in which limb could be saved and excellent functional results achieved.
Limb-saving surgery can be a viable option even in gigantic enormously large musculoskeletal malignancy. Proper counseling, health education, general awareness, and tracking of patients are must to avoid menace to patient limb and life.
Malignant transformation is always a possibility of primary benign looking osteochondromas. Proper counseling at first visit, tracking of patients at regular interval, and timely refer to tertiary care center is paramount to save the limb as well as life.
References
- 1.Richardson RR. Variants of exostosis of the bone in children. Semin Roentgenol 2005;40:380-90. [Google Scholar | PubMed]
- 2.Malghem J, Berg BV, Noël H, Maldague B. Benign osteochondromas and exostotic chondrosarcomas: Evaluation of cartilage cap thickness by ultrasound. Skeletal Radiol 1992;21:33-7. [Google Scholar | PubMed]
- 3.Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008;3:3. [Google Scholar | PubMed]
- 4.Canella P, Gardini F, Boriani S. Exostosis: Development, evolution and relationship to malignant degeneration. Ital J Orthop Traumatol 1981;7:293-8. [Google Scholar | PubMed]
- 5.Altay M, Bayrakci K, Yildiz Y, Erekul S, Saglik Y. Secondary chondrosarcoma in cartilage bone tumors: Report of 32 patients. J Orthop Sci 2007;2:415-23. [Google Scholar | PubMed]
- 6.Kim WJ, Kim KJ, Lee SK, Choy WS. Solitary pelvic osteochondroma causing L5 nerve root compression. Orthopedics 2009;32:922. [Google Scholar | PubMed]
- 7.Wang WY, Du LD, Lv WC, Tian Y, Shao Q, Zhang YH, et al. Osteochondroma of the symphysis pubis: A rare cause of bladder outlet obstruction. Am Surg 2010;76:916-8. [Google Scholar | PubMed]
- 8.Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar | PubMed]
- 9.Evans HL, Ayala AG, Romsdahl MM. Prognostic factors in chondrosarcoma of bone: A clinicopathologic analysis with emphasis on histologic grading. Cancer 1977;40:818-31. [Google Scholar | PubMed]
- 10.Andreou D, Ruppin S, Fehlberg S, Pink D, Werner M, Tunn PU. Survival and prognostic factors in chondrosarcoma: Results in 115 patients with long-term follow-up. Acta Orthop 2011;82:749-55. [Google Scholar | PubMed]
- 11.Available from: htttps://www.guinnessworldrecords.com/world-records/largest-bone tumour [Last accessed on 2016 Sep 14]. [Google Scholar | PubMed]
- 12.Sharma R, Sohal HS, Malhotra N. Mega tumour (chondrosarcoma) of humerus-an insanely large tumor and its social implications. J Orthop Case Rep 2017;7:102-5. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2015 Isolated Proximal Fibular Stress Fracture In Osteoarthritis Knee Presenting As L5 Radiculopathy
July 10, 2015 Isolated Proximal Fibular Stress Fracture In Osteoarthritis Knee Presenting As L5 Radiculopathy September 10, 2021 Type II Odontoid Fractures Case Series: History of Seizures a Risk Factor for Failure of Non-operative Treatment of Type II Odontoid Fractures
September 10, 2021 Type II Odontoid Fractures Case Series: History of Seizures a Risk Factor for Failure of Non-operative Treatment of Type II Odontoid Fractures November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report
November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report June 4, 2021 A Novel “Shark-Fin” Pyramidal Achilles Bone-Tendon Allograft Surgical Technique for Delayed Reconstruction of Triceps Tendon Rupture and Review of the Literature
June 4, 2021 A Novel “Shark-Fin” Pyramidal Achilles Bone-Tendon Allograft Surgical Technique for Delayed Reconstruction of Triceps Tendon Rupture and Review of the Literature