
Perilunate dislocation of the carpus is rare and often goes unnoticed, its bilateral form is even rarer requiring high-energy trauma generally to a wrist in hyperextension and often in ulnar tilt.
Dr. Papa Amadou Ba, Department of Orthopedic and Trauma Surgery, Army Training Hospital Principal, Avenue Nelson Mandéla, B.P. 3006, Dakar, Senegal. E-mail: pabaortho@gmail.com
Introduction: Perilunate dislocations are uncommon injuries requiring high-energy trauma. They are responsible for serious lesions that can compromise the function of the limb. We report a case of pure bilateral perilunate dislocation in a parachutist while landing.
Case Report: The case involved a 30-year-old military officer of special forces who underwent closed trauma to both wrists following an automatic opening parachute jump. He had first consulted a garrison medical center where a wrist sprain had been treated. Given the persistence of the pain, he was referred to our clinic 2 months later. X-rays of the wrists showed bilateral perilunate dislocation, type 1 on the right and type 3 on the left, according to the Witvoët and Allieu classification. Surgery was indicated with 2 open scapholunate and lunotriquetral pins. The post-operative course was simple, with a complete resumption of professional activity after 9 months.
Conclusion: Perilunate dislocations of the carpus are uncommon injuries that often go unnoticed. They can also occur after a parachute landing. Treatment must be surgical.
Keywords: Bilateral, semilunar dislocation, parachutist.
Perilunate dislocations are rare injuries requiring high-energy trauma, generally to a wrist in hyperextension and often in ulnar tilt [1]. They are responsible for serious capsule ligament and osteocartilaginous injuries. However, the simultaneous bilateral form is very rare, with only a few cases reported in the literature [2]. We report a case of pure bilateral perilunate dislocation in a parachutist while landing.
We report the case of a 30-year-old military officer of special forces, with no previous medical history, who underwent closed trauma to both wrists following an automatic opening parachute jump. He missed his landing and would have fallen with a reception on the palms of both hands on the hyperextended wrist. His first consultation was at a garrison medical center, where an X-ray of both wrists was requested. The general practitioner did not see the bone lesion and treated it as a wrist sprain by splinting both wrists and taking painkillers. Given the persistence of the pain, he was referred to our clinic 2 months later. Clinical examination revealed wrists stiffness, slightly flexed, painful, and disabling.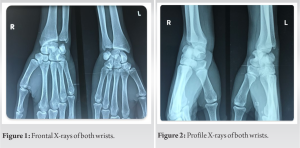 X-rays of the wrists showed disorganization of the carpus and a spinning top appearance of the semilunate on the frontal views (Fig. 1) and bilateral perilunate dislocation on the lateral views (Fig. 2) type 1 on the right and type 3 on the left according to the Witvoët and Allieu classification [3].
X-rays of the wrists showed disorganization of the carpus and a spinning top appearance of the semilunate on the frontal views (Fig. 1) and bilateral perilunate dislocation on the lateral views (Fig. 2) type 1 on the right and type 3 on the left according to the Witvoët and Allieu classification [3].  There were no other associated lesions. Regarding the age of the lesions, we ordered a computed tomography (CT) scan of both wrists (Fig. 3) to establish the diagnosis and rule out necrosis of the semilunate. An indication for surgery was given. The operation was performed under a general anesthetic. The reduction was carried out openly, using a dorsal approach to the wrists and 2 scapholunate and lunotriquetral pins (Fig. 4 and 5).
There were no other associated lesions. Regarding the age of the lesions, we ordered a computed tomography (CT) scan of both wrists (Fig. 3) to establish the diagnosis and rule out necrosis of the semilunate. An indication for surgery was given. The operation was performed under a general anesthetic. The reduction was carried out openly, using a dorsal approach to the wrists and 2 scapholunate and lunotriquetral pins (Fig. 4 and 5).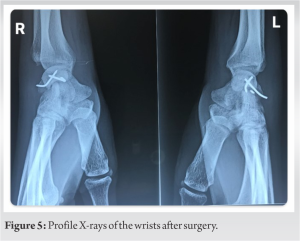 The post-operative course was simple. Wrist splints were applied for 3 weeks and rehabilitation was started in the 3rd week. After 9 months, the patient had regained good function in both wrists (extension: 60°, flexion: 50°) with no pain and had resumed his professional activities.
The post-operative course was simple. Wrist splints were applied for 3 weeks and rehabilitation was started in the 3rd week. After 9 months, the patient had regained good function in both wrists (extension: 60°, flexion: 50°) with no pain and had resumed his professional activities.
Parachuting accidents in the military environment are a small-scale phenomenon when compared to the number of jumps made. This is probably the consequence of the quality of the training, the rigorous training program, the respect of the prevention measures, and the specific selection [4]. Thus the incidence rate of accidents following an automatic opening jump is close to 20 accidents/1000 jumps [5, 6]. Looking more specifically at fractures, the literature records around 2 military officers with at least one bone injury/1000 parachutists [4, 7]. All the studies [6, 7, 8, 9] confirm the preferential involvement of the lower limb. The foot and ankle are particularly at risk [10]. Parachutists will impact the ground on their lower limbs, increasing the risk of trauma at this level. There may also be a pendulum effect. In this case, the parachutist may adopt a “protective” position by putting their hands on the ground to land. Because of the landing position, the upper limb is exposed to trauma. The shoulder remains the joint of the upper limb most affected, with 51.4% of injuries, followed by the wrist and the hand [11]. The most common wrist injury is scaphoid fracture [12], which is often diagnosed at a late stage. It is also important to bear in mind the perilunate dislocation of the carpus, which can occur alone, as in the case of our patient, or association with a fracture. Perilunate dislocations are uncommon and scarce in the literature on jumping accidents. They are most often the result of failure to respect landing positions. In a more recent article, Brickwell and Craig [13] reviewed the literature on injuries in military parachuting and found a rate of wrist dislocation ranging from 0.2% to 0.6% depending on the series. Perilunate dislocation of the carpus is one of the regularly diagnosed in traumatology but misdiagnosed by general practitioners. Diagnosis is missed in 25% [1] of cases, often leading to a delay in treatment. It is a genuine surgical emergency, following a high-energy trauma. Its mechanism is hyper-extension associated with torsion, ulnar inclination, and intra-carpal supination [14]. It is a severe injury because of the complexity of the carpal joint. They may be posterior (the most common) or anterior, depending on the displacement of the distal segment. In 60% of cases, the fracture is a dislocation rather than a pure perilunate dislocation. The clinical examination is poor, as there is virtually no wrist deformity, often masked by rapid onset locoregional edema. However, the intense pain and total functional impotence should arouse attention. A deficit in the median nerve territory should be systematically sought, given the possibility of compression of the carpal tunnel by the semilunaris. As the frontal X-ray is often misleading, a detailed analysis of the profile X-ray is essential to make a precise diagnosis. A CT scan, without delaying surgical management, will provide an exhaustive assessment of the injury. Early surgical treatment by reducing the dislocation using external maneuvers will determine the functional prognosis. The aim of treatment is twofold: To restore function (mobility, pain) and to prevent the onset of post-traumatic osteoarthritis. Treatment by osteosynthesis will complete this procedure, followed by a period of immobilization that varies according to the extent of the ligament and bone damage.
Perilunate dislocation of the carpus is an uncommon traumatic injury. They occur in high-energy trauma. They can also occur after a parachute landing without being part of a polytrauma. They often go unnoticed and the risk in the event of late or even inappropriate treatment is the evolution toward sequelae instability of the carpus linked to the early degenerative process severely impacting the functional future of the wrist in an often young patient.
Bilateral carpal perilunate dislocation is a very rare condition. It is exceptional during parachute jump accidents. Diagnosis is often difficult. As the frontal X-ray is often misleading, a detailed analysis of the profile X-ray is essential to make a precise diagnosis. We must think of this traumatological entity in front of any pain in the wrist after a parachutist jump incident.
References
- 1.Herzberg G, Comtet JJ, Linscheid RL, Amadio PC, Cooney WP, Stalder J. Perilunate dislocations and fracture-dislocations: A multicenter study. J Hand Surg Am 1993;18:768-79. [Google Scholar]
- 2.Zonoozi E, Mazhar FN, Khazai M, Nejadgashti N. Bilateral volar lunate dislocation-a rare case report. J Res Med Sci 2009;14:187-90. [Google Scholar]
- 3.Allieu Y. Medical-Surgical Encyclopedia, Locomotor device. Technical Ed.; Paris: 1987. Carpal sprains, subluxations and dislocations; p. 14046. C-IO, 9. [Google Scholar]
- 4.Bricknell MC. Is service with the parachute regiment bad for your health? Occup Med (Lond) 1999;49:79-84. [Google Scholar]
- 5.Ekeland A. Injuries in military parachuting: A prospective study of 4499 jumps. Injury 1997;28:219-22. [Google Scholar]
- 6.Mayet A, Bay C, Salivas A, Verret C. Parachuting accidents in airborne units in the south-west land region 2004-2005. Army Med 2009;37:3-9. [Google Scholar]
- 7.Hallel T, Naggan L. Parachuting injuries: A retrospective study of 83,718 jumps. J Trauma 1975;15:14-9. [Google Scholar]
- 8.Bricknell MC, Amoroso PJ, Yore MM. What is the risk associated with being a qualified military parachutist? Occup Med (Lond) 1999;49:139-45. [Google Scholar]
- 9.Vannoni M. Traumatologie du Parachutisme. Statistiques à Propos de 1300000 Sauts. Thèse Médecine Toulouse; 1971. [Google Scholar]
- 10.Tripon P, Renault J, Becker JM, Rochat G. Limb trauma during parachuting. Ann Chir 1990;44:493-8. [Google Scholar]
- 11.Bertrand L, Facione J, Chappus JJ, Lagauche D. Upper limb traumatic accidents among French paratroopers. A review of 266 accidents which occurred at the paratrooper school between 2000 and 2007. Army Med 2013;41:181-90. [Google Scholar]
- 12.Samy J, Queyran X, Aigle L. Fractures induced by the automatic opening jump: Study of the injured over 4 years and 44,000 jumps followed at the medical center of the armies of Calvi. Army Med 2014;42:163-70. [Google Scholar]
- 13.Bricknell MC, Craig SC. Military parachuting injuries: A literature review. Occup Med (Lond) 1999;49:17-26. [Google Scholar]
- 14.Murray PM, Palmer CG, Shin AY. The mechanism of ulnar-sided perilunate instability of the wrist: A cadaveric study and 6 clinical cases. J Hand Surg Am 2012;37:721-8. [Google Scholar]



