
Triceps tendon avulsion is a rare tendinous injury. If left untreated, such injuries can lead to a weakening of the patient's arm and cause significant disability. However, this can be avoided with appropriate diagnosis and early surgical intervention.
Dr. Abhijit Bandyopadhyay, University Department of Orthopaedic and Trauma Surgery, Tort Centre, Ninewells Hospital, Dundee, Scotland. E-mail: abhi_34358@rediffmail.com
Introduction: Triceps tendon avulsion is a rare tendinous injury that can be easily overlooked. If left untreated, such injuries can lead to a weakening of a patient’s elbow extension and thereby cause significant disability; therefore, early identification and appropriate surgical intervention are important.
Case Report: We report bilateral triceps tendon avulsion injuries in a 49-year-old, right-hand dominant airline pilot. The patient fell while running and injured both his elbows. X-rays of both elbows showed displaced olecranon avulsion fractures, confirming triceps tendon injuries. Bone tendons were repaired with the suture anchor technique, and a solid repair was achieved. 3 months post-surgery, the post-operative progress of the patient was satisfied with full function, a range of motion of 5–150° on the left arm, and 0–150° on the right arm and ability to return to work with no restrictions.
Conclusion: Triceps tendon avulsion is a rare injury with few reported cases. Literature suggests that the successful outcome of the patient depends on early identification and timely intervention, such as surgical repair through a trans-osseous suture technique. Our report adds to the knowledge base available in the existing medical literature for future reference by healthcare professionals.
Keywords: Triceps, tendon, avulsion, surgical repair.
Triceps tendon avulsion is a rare injury [1], and concomitant elbow injuries with avulsion of the triceps tendon are even rarer [2]. Untreated cases can lead to significant disability, and there is currently no standard or universally accepted protocols for such injuries. Here, we report a case of a 49-year-old patient with a bilateral triceps tendon avulsion injury. While several factors can contribute to triceps tendon avulsion, it is important to consider potential underlying causes, such as anabolic steroid intake, as they may play a role in the development of this condition. However, the specific cause of the triceps tendon avulsion in the presented case was not explicitly recorded in the patient’s medical history. It is worth noting that anabolic steroid use has been associated with tendon injuries in some studies [3, 4]. Therefore, it is plausible to consider anabolic steroid intake as a potential contributing factor in this case.
A 49-year-old male presented to the Accident and Emergency Department with bilateral elbow pain following a fall while running on ice. The patient is fit and well, takes no regular medication, and is a right-handed dominant pilot. On clinical examination, there was no swelling or deformity present. He had full extension of the left arm and lacked 20° of extension of the right arm. He had significant weakness in the extension of both elbows, and his active function was limited by pain on both sides. Plain radiographs revealed bilateral olecranon avulsion fractures, confirming triceps tendon avulsion injuries (Fig. 1).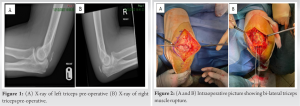 The patient also had a non-displaced fracture of the right radial head. Although the specific cause of the triceps tendon avulsion was not explicitly recorded in the patient’s medical history, it is worth considering potential underlying factors such as anabolic steroid use, which has been associated with tendon injuries in some cases. Further investigation into the patient’s history and potential risk factors could provide valuable insights into the etiology of this injury. The patient underwent bilateral open fixation using the suture technique 10 days post-injury. Ruptured bilateral triceps were noted, the left more severe than the right. Tourniquet time was 43 min (each side) at 250 mmHg. A midline incision curved radially was used to expose the triceps, protecting the ulnar nerve throughout. A suture-only repair with sutures and non-metallic suture anchors on each side was undertaken (Fig. 2). Once the repair was complete, both elbows were moved to the full range of motion (ROM) to check the adequacy of the repair and ROM. Wound closure was done in layers with 3/0 Monocryl and Steri-Strips™ applied to the skin. Bilateral back slabs to 45° were applied, leaving the wrist free. The patient was discharged home the day after surgery with appropriate analgesia. The patient was changed into a lightweight back slab at 45° 1 week postoperatively. Three weeks postoperatively, the wounds had healed well, and radiographs revealed a good position of the repair (Fig. 3).
The patient also had a non-displaced fracture of the right radial head. Although the specific cause of the triceps tendon avulsion was not explicitly recorded in the patient’s medical history, it is worth considering potential underlying factors such as anabolic steroid use, which has been associated with tendon injuries in some cases. Further investigation into the patient’s history and potential risk factors could provide valuable insights into the etiology of this injury. The patient underwent bilateral open fixation using the suture technique 10 days post-injury. Ruptured bilateral triceps were noted, the left more severe than the right. Tourniquet time was 43 min (each side) at 250 mmHg. A midline incision curved radially was used to expose the triceps, protecting the ulnar nerve throughout. A suture-only repair with sutures and non-metallic suture anchors on each side was undertaken (Fig. 2). Once the repair was complete, both elbows were moved to the full range of motion (ROM) to check the adequacy of the repair and ROM. Wound closure was done in layers with 3/0 Monocryl and Steri-Strips™ applied to the skin. Bilateral back slabs to 45° were applied, leaving the wrist free. The patient was discharged home the day after surgery with appropriate analgesia. The patient was changed into a lightweight back slab at 45° 1 week postoperatively. Three weeks postoperatively, the wounds had healed well, and radiographs revealed a good position of the repair (Fig. 3).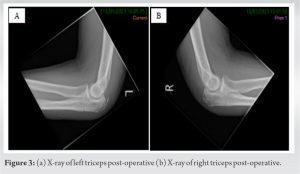 The ROM on the left side was 5–85°, and on the right side, it was 0–90°. We advised the patient to start moving his elbows at 3 weeks, but he was advised to avoid heavy lifting, pushing, and pulling for a further 3 weeks. The patient required splints to be worn outdoors and overnight for 3 weeks. After this period, the splints were discarded and formal physiotherapy commenced, with ROM increasing for 5–145° on the right side and 30–130° on the left side. At 3 months postoperatively, he gained full ROM in the right arm (0–150°) and nearly full ROM in the left arm (5–150°) and returned to work at full capacity.
The ROM on the left side was 5–85°, and on the right side, it was 0–90°. We advised the patient to start moving his elbows at 3 weeks, but he was advised to avoid heavy lifting, pushing, and pulling for a further 3 weeks. The patient required splints to be worn outdoors and overnight for 3 weeks. After this period, the splints were discarded and formal physiotherapy commenced, with ROM increasing for 5–145° on the right side and 30–130° on the left side. At 3 months postoperatively, he gained full ROM in the right arm (0–150°) and nearly full ROM in the left arm (5–150°) and returned to work at full capacity.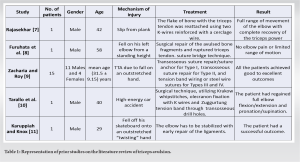
Triceps tendon avulsion is a rare tendinous injury (accounting for 1–2% of all tendon injuries), and it is considered the least common among all tendon injuries. As a result, misdiagnosis and neglect are frequent, which can result in long-term functional disability [1]. Early identification and surgical repair are essential. This diagnosis should be considered in patients presenting with pain and swelling at the elbow posteriorly after a traumatic injury, most commonly after a fall onto an outstretched hand. It can occur after direct or indirect trauma, generally at the osseo-tendinous junction. Clinical symptoms include a palpable gap in tendon continuity, swelling, tenderness, and the inability to extend the affected joint. A ‘flake’ fracture on lateral radiographs can help in the diagnosis [5]. Literature suggests that successful patient outcome depends on early identification and timely intervention, such as surgical repair through a trans-osseous suture technique using the Krakow method [1]. In addition to traumatic causes, it is important to consider other potential factors that may contribute to triceps tendon avulsion, including anabolic steroid use, which has been reported to be associated with tendon injuries in some cases [6]. Further research and consideration of the patient’s medical history could provide valuable insights into the etiology of this rare injury. There are very few case reports and even fewer studies reported in the medical literature (Table 1). It has been reported that triceps tendon ruptures and avulsions are often associated with systemic diseases. One case report illustrated a unique case of a 20-year-old female patient with pseudohypoparathyroidism who sustained bilateral triceps avulsion fractures after a fall. The patient underwent suture anchor fixation, augmented with tension band suture as a double row repair, with excellent post-operative results [12]. After reviewing the radiographs of our patient, we observed bilateral avulsion fractures with displacement of the bony fragments, as shown in Fig. 1. Considering his fitness level and employment as a pilot, as well as the presence of bilateral injuries, we concluded that surgical fixation would be beneficial. Consequently, we opted to perform surgery on both elbows during the same surgical session. This approach was chosen to ensure that the patient’s rehabilitation time would be equal for both elbows and to avoid any delays in performing surgery on the contralateral elbow. These are very rare injuries, and they are extremely rare bilaterally. The risks of surgery include infection (1–2%), neurovascular injury (ulnar nerve), stiffness, re-tear (20%), stiffness of the elbow, and complex pain. The typical approach to repairing a ruptured triceps tendon is to reattach it using drill holes in the olecranon. Alternative techniques include reattaching the tendon to the olecranon via a periosteal flap or an intraosseous anchor. However, in some cases where there is a reasonably-sized avulsed flake of bone from the tendon’s insertion on the olecranon, fixation using Kirschner wires (K-wires) and a tension band may be considered a viable option [7]. While the chosen surgical technique in this case report involved suture-only repair with non-metallic suture anchors, it is important to consider alternative techniques depending on the specific characteristics of the injury and the patient’s individual factors. Moreover, the presence of potential underlying causes such as anabolic steroid use should be taken into account when determining the most suitable surgical approach. The suture anchor technique is not frequently used for primary repair. However, when employed, suture anchors are inserted into the middle of the tendon footprint and secured to locking stitches made on both sides of the tendon. In our case, we used bilateral open fixation with suture anchor technique to repair a triceps tendon avulsion injury, which provided satisfactory outcomes. During surgical treatment, we opted for a repair of the triceps tendon using soft anchors, which were drilled into the top of the olecranon to enable the tendon to be anchored at its original insertion point. These anchors are designed to require smaller drill holes and offer comparable, if not superior, strength to much longer anchors. Consequently, they necessitate less bone removal, permit multiple points of fixation when anchoring soft tissue to bone, and offer high pull-out strength. Similar to our study, Furuhat et al. [8] used the suture technique on a 58-year-old male and showed better outcomes with recovery in the ROM as well as complete pain and discomfort recovery. In line with these findings, Mancini et al. [13] performed open fixation surgery for bilateral triceps tendon avulsion injuries and reported better outcomes with recovery in the ROM as well as complete pain and discomfort recovery. However, the period of recovery was 5–9 months in the previous studies, which is longer than our study (3 months). We suggest that our study will enhance the knowledge available in the existing medical literature and simplify the identification and treatment of similar injuries for healthcare professionals in the future. Furthermore, the reporting of such cases will contribute to the development of standardized protocols and guidelines for the recognition and management of these rare conditions.
We report a case of bilateral triceps tendon avulsion injuries in a 49-year-old patient with a successful outcome after surgical intervention. Triceps tendon avulsion is a rare injury with few reported cases. If left untreated, they can lead to a significant disability. Our case will add to the knowledge of existing literature and will improve the management of such injuries in the future.
Triceps tendon avulsion is a rare tendinous injury. If left untreated, such injuries can lead to a weakening of the patient’s arm and cause significant disability. However, this can be avoided with an appropriate diagnosis and early surgical intervention.
References
- 1.Sharma P, Vijayargiya M, Tandon S, Gaur S. Case report: Triceps tendon avulsion: A rare injury. Ethiop J Health Sci 2014;24:97. [Google Scholar]
- 2.Canbora K, Ozyurek S, Gumussuyu G, Kose O. Triceps tendon avulsion and associated injuries of the elbow. Case Rep 2013;2013:bcr201300946. [Google Scholar]
- 3.Harris PC, Atkinson D, Moorehead JD. Bilateral partial rupture of triceps tendon. Am J Sports Med 2004;32:787-92. [Google Scholar]
- 4.Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med 2004;32:431-4. [Google Scholar]
- 5.Vannabouathong C, Ayeni OR, Bhandari M. A narrative review on avulsion fractures of the upper and lower limbs. Clin Med Insights Arthritis Musculoskelet Disord 2018;11:117954411880905. [Google Scholar]
- 6.Golshani B, Bindra J, Hunter JC. Bilateral triceps tendon tear. Radiol Case Rep 2011;6:581. [Google Scholar]
- 7.Rajasekhar C. Avulsion of the triceps tendon. Emerg Med J 2002;19:271-2. [Google Scholar]
- 8.Furuhata R, Kamata Y, Kono A, Nishimura T, Otani S, Morioka H. Surgical repair using suture bridge technique for triceps tendon avulsion. Case Rep Orthop 2021;2021:1-4. [Google Scholar]
- 9.Zacharia B, Roy A. A clinicoradiological classification and a treatment algorithm for traumatic triceps tendon avulsion in adults. Chin J Traumatol 2021;24:266-72. [Google Scholar]
- 10.Tarallo L, Zambianchi F, Mugnai R, Costanzini CA, Catani F. Distal triceps tendon repair using Krakow whipstitches, K wires, tension band and double drilling technique: A case report. J Med Case Rep 2015;9:36. [Google Scholar]
- 11.Karuppiah SV, Knox D. Elbow dislocation with complete triceps avulsion. Case Rep Orthop 2014;2014:1-3. [Google Scholar]
- 12.Najefi AA, Domos P. A unique case of bilateral triceps avulsion fracture in a patient with pseudohypoparathyroidism. Shoulder Elb 2021;13:334-8. [Google Scholar]
- 13.Mancini F, Bernardi G, De Luna V, Tudisco C. Surgical repair of isolated triceps tendon rupture using a suture anchor technique: A case report. Joints 2016;4:250-2. [Google Scholar]





