
• Adherence of polyurethane foam is unusual complication of VAC therapy. • Adherence of foam is different from missed retained sponges.
Dr. Shahnawaz Khan, Department of Orthopaedics, All India Institute of Medical Sciences, Bhubaneswar, Odisha, India. E-mail: skhanortho2022@gmail.com
Introduction: Vacuum-assisted closure (VAC) dressings are used for many indications nowadays in wound management. However, there are complications with VAC dressings also. In this study, we report a 44-year-old patient with a vertical shear injury with post-operative wound complication of adherent polyurethane sponge over her wound which was removed by piecemeal dissection.
Case Report: A 44-year-old patient sustained a vertical shear pelvic injury following which spinopelvic fusion surgery was performed. The patient developed wound dehiscence along with discharge on POD 4. Following this, VAC dressing was applied to the wound. After 3 days, the polyurethane sponge became adherent to the wound. The sponge was removed gradually through daily debridement in a piecemeal manner. The wound was found to be healthy and a keystone flap was raised to cover the wound.
Conclusion: Although such complication of an adherent sponge has not been reported to date, one must keep in mind this complication while making improvisations to commercially available VAC dressings.
Keywords: Vacuum-assisted closure, negative pressure wound treatment, wound closure, retained, polyurethane.
Negative pressure wound treatment (NPWT) or vacuum-assisted closure (VAC) is a non-surgical means for modulating wound healing [1]. Ever since first proposed by Argenta and Morykwas in 1997 [2], the application has found widespread use in managing acute/chronic wounds. The exact mechanism of functioning of VAC is still unclear. However, it is believed that foam sponges are used to fill the wound void and negative pressure reduces edema, reduces the local bacterial load, and improves local blood flow thereby promoting granulation tissue ingrowth [1, 3]. The VAC system has yielded great results. However, there are complications also [4, 5, 6]. We present to you a rare complication in which the polyurethane sponge got adhered to the floor of a wound over the sacral region following VAC dressings that could not be removed easily.
A 44-year-old female came to us 1 year ago with a history of road traffic accident. She complained of pain in the lower back region. On examination, her vitals were stable. The pelvic compression test was positive and there was a limb length discrepancy. Radiographs revealed a vertical shear pelvis (Fig. 1). We planned for spinopelvic fusion surgery with anterior reconstruction of the pelvic ring. In the supine position, the symphyseal plating was done through an anterior approach. Then, the patient was flipped to prone position and a midline incision over the sacrum was applied followed by soft-tissue dissection. Pedicle screws were inserted from L4 to the ilium and rod was connected after the fracture was reduced. This was also supplemented with a buttress sacral plate (Fig. 2a-c). However, she started having a discharge from the wound on 4th day in the post-operative period. The wound was opened and VAC dressing was applied as shown in Fig. 2d. In the absence of a commercial VAC device, the suction was connected to the wall-mounted suction. The dressing was changed on the 3rd day. However, it was noticed that a part of the polyurethane sponge was found to be adherent to the wound base (Fig. 3a). All attempts to remove the retained sponge failed and daily debridement and piecemeal removal was done. The patient was taken to our minor operating room daily and the parts of the adherent sponge that loosened out were removed using a 15-number surgical blade. The wound was irrigated with normal saline after the minor surgery and was covered. Everyday, the wound was dressed twice. Subsequently, by 2 weeks, the entire sponge was removed and the wound was found to be healthy and had developed a layer of granulation tissue (Fig. 3b).
We planned for spinopelvic fusion surgery with anterior reconstruction of the pelvic ring. In the supine position, the symphyseal plating was done through an anterior approach. Then, the patient was flipped to prone position and a midline incision over the sacrum was applied followed by soft-tissue dissection. Pedicle screws were inserted from L4 to the ilium and rod was connected after the fracture was reduced. This was also supplemented with a buttress sacral plate (Fig. 2a-c). However, she started having a discharge from the wound on 4th day in the post-operative period. The wound was opened and VAC dressing was applied as shown in Fig. 2d. In the absence of a commercial VAC device, the suction was connected to the wall-mounted suction. The dressing was changed on the 3rd day. However, it was noticed that a part of the polyurethane sponge was found to be adherent to the wound base (Fig. 3a). All attempts to remove the retained sponge failed and daily debridement and piecemeal removal was done. The patient was taken to our minor operating room daily and the parts of the adherent sponge that loosened out were removed using a 15-number surgical blade. The wound was irrigated with normal saline after the minor surgery and was covered. Everyday, the wound was dressed twice. Subsequently, by 2 weeks, the entire sponge was removed and the wound was found to be healthy and had developed a layer of granulation tissue (Fig. 3b).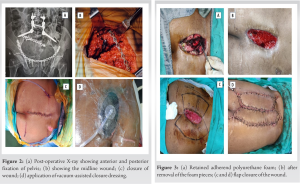 A keystone perforator flap was done to close the defect as shown in Fig. 3c-d. The patient was made to bear weight after 2 months of surgery with the help of a walker. Full weight-bearing without aids was started 4 months after the surgery. After 1 year of follow-up, the patient is doing fine and can walk without any aids. The wound has healed and there are no wound complications (Fig. 4).
A keystone perforator flap was done to close the defect as shown in Fig. 3c-d. The patient was made to bear weight after 2 months of surgery with the help of a walker. Full weight-bearing without aids was started 4 months after the surgery. After 1 year of follow-up, the patient is doing fine and can walk without any aids. The wound has healed and there are no wound complications (Fig. 4).
The use of VAC dressings has been rising in medical practice due to a variety of applications. However, the dressings are costly and cannot be afforded by people of lower socioeconomic class in a developing country like ours. As a result, numerous improvisations have taken place by different people to make them affordable. In most cases, these improvisations work causing great benefit to the patients. However, in some cases, complications do occur. These include failure of the VAC system, allergies to the adhesive drape, excoriation of the skin, bleeding and uncontrolled sepsis, toxic shock syndrome, and retention of sponges [1, 7, 8, 9]. Beral et al. reported a case of retained sponge that was missed during removal and subsequently required another surgery for removal [10]. A retained sponge can itself become a source of purulent discharge and need to be extracted as mentioned by Dessy et al. [11] Most of the case reports in the literature have shown us that the sponge was retained in the abdominal cavity. One case report by Fox et al. showed the presence of a retained sponge in the sacral wound which subsequently became infected [4]. The incidence of retained sponges has been reported to be around 1 in 3000 cases [12]. However, the “retained sponges” are different from the “adherent sponge” [6, 8, 9]. Being a rare complication, such a scenario is not reported. A retained sponge is often a forgotten foreign body left in the wound which comes to notice after getting infected or complicated. However, this was not the case in our setup. In our case, the sponge got stuck to the wound after the removal of the negative suction. Adherent polyurethane foam to the underlying tissue is a challenge to remove and may require repeated debridement for removal. Luckily, in our case, there was no infection and the wound improved with time. VAC therapy is a closed-loop system in which the negative pressure can be applied either as a continuous or intermittent cycle. The optimum pressure ranges from 25 to 250 mmHg depending on the wound situation [7, 13]. Polyurethane foam adherence has been encountered at a pressure level between 100 and 125 mmHg [11]. The wall-mounted suction is a continuous system and an inadvertent increase in pressure for a long duration (2–3 days) could be responsible for adherence foam in our case. Due to persistence of the abnormal pressures, the sponge got stuck to the wound. The pressure in a wall-mounted suction system in a hospital is regulated centrally and is affected by various parameters. Hence, the accurate monitoring of the pressure is necessary at frequent intervals. The only way to overcome this situation is to avoid making improvisations to the commercially available VAC systems. Such a rare complication also requires proper tissue handling. Improper handling of the tissues will lead to damage to the healthy granulation tissue which will impair the wound healing. A keystone perforator flap is a fasciocutaneous flap which is described for coverage of such large wounds and obviates the need for any microvascular surgery or any skin grafts [14]. It is cosmetically accepted by a large section of people [14, 15, 16]. However, the complication of scar formation exists in this kind of flaps [14]. Similar scar was seen in our case also. Since the skin in the sacral area remains covered by the clothing, we went ahead with the plan of a Keystone flap in this region.
One must be cautious and take extra precautions while making improvisations to the VAC system. Pressure should be checked at frequent intervals to prevent such complications. While doing the piecemeal removal of sponges, one needs to be very careful to avoid the retention of sponges. One must keep in mind such a rare complication while making improvisations to the commercially available VAC systems. Prompt removal of the retained or adherent sponge is paramount to control infections. If required, the patient can be kept under the cover of antibiotics while the VAC is applied.
Although this complication of adherent sponge has not been published in literature, one must keep in mind this complication while making improvisations to commercially available VAC dressings.
References
- 1.Agarwal P, Kukrele R, Sharma D. Vacuum assisted closure (VAC)/negative pressure wound therapy (NPWT) for difficult wounds: A review. J Clin Orthop Trauma 2019;10:845-8. [Google Scholar]
- 2.Argenta LC, Morykwas MJ. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann Plast Surg 1997;38:563-76; discussion 577. [Google Scholar]
- 3.Genecov DG, Schneider AM, Morykwas MJ, Parker D, White WL, Argenta LC. A controlled subatmospheric pressure dressing increases the rate of skin graft donor site reepithelialization. Ann Plast Surg 1998;40:219-25. [Google Scholar]
- 4.Fox A, Tadros A, Perks AG. An unusual complication of Vacuum Assisted Closure in the treatment of a pressure ulcer. J Wound Care 2004;13:344-5. [Google Scholar]
- 5.Jones GA, Butler J, Lieberman I, Schlenk R. Negative-pressure wound therapy in the treatment of complex postoperative spinal wound infections: Complications and lessons learned using vacuum-assisted closure. J Neurosurg Spine 2007;6:407-11. [Google Scholar]
- 6.Gwan-Nulla DN, Casal RS. Toxic shock syndrome associated with the use of the vacuum-assisted closure device. Ann Plast Surg 2001;47:552-4. [Google Scholar]
- 7.Stal S, Serure A, Donovan W, Spira M. The perioperative management of the patient with pressure sores. Ann Plast Surg 1983;11:347-56. [Google Scholar]
- 8.Ploumis A, Mehbod AA, Dressel TD, Dykes DC, Transfeldt EE, Lonstein JE. Therapy of spinal wound infections using vacuum-assisted wound closure: Risk factors leading to resistance to treatment. J Spinal Disord Tech 2008;21:320-3. [Google Scholar]
- 9.Saeed MU, Kennedy DJ. A retained sponge is a complication of vacuum-assisted closure therapy. Int J Low Extrem Wounds 2007;6:153-4. [Google Scholar]
- 10.Beral D, Adair R, Peckham-Cooper A, Tolan D, Botterill I. Chronic wound sepsis due to retained vacuum assisted closure foam. BMJ 2009;338:b2269. [Google Scholar]
- 11.Dessy LA, Serratore F, Corrias F, Parisi P, Mazzocchi M, Carlesimo B. Retention of polyurethane foam fragments during VAC therapy: A complication to be considered. Int Wound J 2013;12:132-6. [Google Scholar]
- 12.Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med 2003;348:229-35. [Google Scholar]
- 13.Gupta RC, Canerdy TD, Skaggs P, Stocker A, Zyrkowski G, Burke R, et al. Therapeutic efficacy of undenatured Type-II collagen (UC-II) in comparison to glucosamine and chondroitin in arthritic horses. J Vet Pharmacol Ther 2009;32:577-84. [Google Scholar]
- 14.Bhat SP. Keystone flaps in coloured skin: Flap technology for the masses? Indian J Plast Surg 2013;46:36-47. [Google Scholar]
- 15.Byun IH, Kim CW, Park TH. The modified keystone flap for pressure ulcers: A modification of the keystone flap with rotation and advancement. Ann Plast Surg 2019;82:299-303. [Google Scholar]
- 16.Rao AL, Janna RK. Keystone flap: Versatile flap for reconstruction of limb defects. J Clin Diagn Res 2015;9:PC05-7. [Google Scholar]







