
Iatrogenic coracoid graft fractures during arthroscopic Latarjet procedure can be salvaged maintaining the triple effect of the Latarjet – the bone block effect, the sling effect, and capsulolabral effect.
Dr. Pramod Kumar Mohan, Department of Shoulder and Sports Injury, Bangalore Shoulder Institute, Bengaluru, Karnataka, India. E-mail: pramod.stanley@gmail.com
Introduction: We present a case report of an iatrogenic conjoint tendon avulsion fracture following arthroscopic Latarjet and salvage technique to address the complication with a novel double sling technique.
Case Report: A 16-year-old male patient who presented with recurrent instability of the right shoulder was counseled for an arthroscopic Latarjet procedure, taking account of critical glenoid bone loss and his contact sporting activities. An intraoperative coracoid tip fracture occurred, which was managed with the double sling technique. At 1-year follow-up, the patient has made a good recovery with a full range of movements and a stable shoulder; the CT scans showed a well-approximated coracoid tip fragment.
Conclusion: Iatrogenic intraoperative coracoid graft fractures during arthroscopic Latarjet can be managed depending on the site of the fracture and quality of the bone. The double sling fixation technique helps in maintaining the sling action of the conjoint tendon in patients with recurrent instability.
Keywords: Latarjet, Coracoid graft fracture, Arthroscopy, Shoulder surgery, Instability, Graft salvage.
Arthroscopic Latarjet is technically demanding and has a steep learning curve providing good union rates and minimal complications with less bleeding, less post-operative pain, and can also deal with associated shoulder pathology and better cosmesis [1]. The complications of arthroscopic Latarjet are similar to those of open Latarjet and include neurovascular complications due to its proximity, graft-related complications, implant-related complications, stiffness, and infection [2, 3]. Athwal et al. have described intraoperative graft fracture in their list of complications but post-operative graft failure has been rarely described [4]. We present a case report of an iatrogenic conjoint tendon avulsion fracture following arthroscopic Latarjet and a novel double sling technique to salvage the coracoid graft.
A 16-year-old male patient who was a college basketball player presented with recurrent anterior shoulder instability of the right shoulder for the past 2 years. He had multiple episodes of dislocation; the most recent episode was 1 month before he presented to us. On clinical examination, the patient had a full range of motion and had a positive apprehension test for instability. Radiological screening with CT and MRI showed glenoid bone loss of 20% and engaging Hill Sachs lesions (Fig. 1). Considering the critical glenoid bone loss with engaging Hill Sach lesion and being a contact sport athlete, he was counseled for arthroscopic Latarjet procedure with remplissage of the Hill Sach lesion.
Considering the critical glenoid bone loss with engaging Hill Sach lesion and being a contact sport athlete, he was counseled for arthroscopic Latarjet procedure with remplissage of the Hill Sach lesion.
Surgical technique
Patient positioning and portal placement
Under general anesthesia and an interscalene block, the patient is positioned in a beach chair position. The arm is prepped and draped held by traction cable with the shoulder in 60° anterior elevation, 10° shoulder abduction and neutral rotation (Fig. 2).
Portal placement (Fig. 2)
A portal: Standard posterior portal known as soft spot, 2 cm medial and inferior from the posterolateral corner of the acromion. Used for visualization and passing switching stick for subscapularis split.
E portal: In the rotator interval, made with the outside-in technique just above the lateral half of the subscapularis.
D portal: Lateral portal made anterior to the long head of the biceps. Used for instruments during coracoid preparation and coracoid osteotomy. Furthermore, used for visualization during the shoulder’s anterior access, exposure, subscapularis split, and fixation of the graft.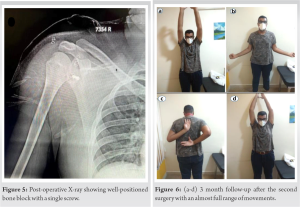
H Portal: Anterosuperior portal above coracoid. Used for coracoid drilling and coracoid osteotomy.
J portal: Anteroinferior portal above subscapularis. Used for visualization during the preparation, osteotomy, and transfer of the coracoid graft.
I portal: Ancillary portal. Used to make the subscapularis split, also used for visualization during the preparation of the coracoid holes.
M portal: Anterior portal made medial to the conjoint tendon. Used for the pectoralis minor tendon release and double-barrel coracoid positioning cannula.
Surgical steps
The arthroscopic Latarjet procedure as described by Lafosse was performed. Remplissage of the Hill Sach lesion was performed with a triple-loaded all-suture anchor (Stryker, India). The coracoid graft was prepared, osteotomized, and transferred through the subscapularis split. The coracoid graft fixation was carried out with two cannulated metal screws (Depuy-Mitek) and tightening of the screws was performed. While tightening the alpha screw, we encountered an iatrogenic fracture of the coracoid graft below the alpha screw causing a free floating fracture of the distal tip of the coracoid graft along with the conjoint tendon (Fig. 3). The alpha screw was removed with the MITEK arthrolatarjet screwdriver. Refixation of the conjoint tendon with the inferior coracoid tip was done with a novel double sling technique. The conjoint tendon was secured with cinch sutures using a fiber wire loaded on the Arthrex scorpion suture passer at the proximal aspect of the conjoint tendon and traction load was given to the proximal suture sling. The conjoint tendon along the bone fragment was approximated to the remaining bone block. Second sling fixation was done using a similar technique, cinch sutures are taken distally to the initial sutures and anchored at 5.30 O’clock position using push-lock while maintaining traction on the proximal suture sling. The proximal suture sling was anchored to the 3.30 O’clock position. (Fig. 4a-d) shows the animated surgical technique of double sling fixation of graft fracture fixation. Intraoperatively fractured coracoid tip, along with conjoint tendon was found stable as the shoulder is put through all range of movements (Video 1). (Fig. 5) shows a post-operative X-ray showing a well-positioned bone block with a single screw. Post-surgery, the patient was immobilized for 2 weeks and rehabilitation was started gradually as per standard protocol followed for arthroscopic Latarjet.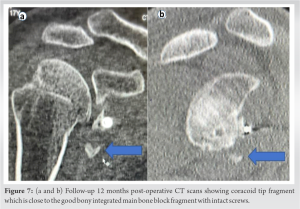
Outcome
The patient was followed up at 3 months and 6 months. At end of the 3-month follow-up visit, the patient had full ROM and no instability. (Fig. 6a-d) shows 3-month follow-up after the surgery with an almost full range of movements. Follow-up CT scan at 12 months after surgery showed good bony integration of the main coracoid graft and intact screw, with the fractured coracoid graft close to the main bone block. The proximity of the coracoid tip fragment implied the sling action of the conjoint tendon was maintained (Fig. 7a). The patient was allowed to return to sports at end of 6 months. The patient has continued to do well at 12-month post-operative with no instability (Fig. 7b).
The arthroscopic Latarjet procedure is well described by Lafosse and has been practiced around the world by many shoulder surgeons. Arthroscopic Latarjet provides excellent visualisation of neurovascular structures and graft positioning, also other shoulder pathologies can be addressed simultaneously [5]. Complication rates following arthroscopic Latarjet by Atwal et al. were similar to open Latarjet case series by Shah et al. [2]. Meraner et al. in his study of a 10-year follow-up of the arthroscopic Latarjet procedure estimated the complication rates to 30% [6]. Pereira and Gutierres in their study of complications of coracoid transfer procedures described a higher percentage of screw-related complications and revision surgeries when compared to data reported in the literature [7]. They highlighted that the arthroscopic technique was found to have an overall lower rate of complications when compared to open procedures. The most commonly described complication is loss of external rotation found in 67% of the shoulders [7]. Athwal et al. described six cases of intraoperative graft fracture, they believed that this complication is preventable with good preparation of the graft under surface to match the glenoid surface. Four out of six cases healed without complication, while two cases needed revision with iliac crust bone block procedures. We believe that the iatrogenic conjoint tendon avulsion fracture of the coracoid graft in this patient is caused by excessive tightening of the alpha screw near the physis close to the conjoint tendon origin. The apophyseal injuries of the base are more common in the age group of 15–16 years in a study by Ogawa et al. [8]. Ogawa’s functional classification of coracoid fractures is fracture of coracoid proximal to coracoclavicular ligament and fracture of coracoid distal to the coracoclavicular ligament [9]. Management of these graft fractures depends on the location of the fracture, the size, stability, and bone quality of the bone block. Fractures at the tip and the level of the alpha screw can be managed with the double sling technique as described in this case report. Fractures between alpha and beta screws can be managed depending on the stability of the bone block and can be left alone in case of adequate stability or managed with a mini buttress plate (Di Giacomo plate; Arthrex)-screws inserted through the plate to get adequate stability [10]. Fractures at the level of beta screws can be managed with a single screw similar to the modified Bristow technique [11]. Fractures above the level of the beta screw are rare and can be managed with the excision of the fragment [4]. Fractures of the longitudinal split of the coracoid bone block can be managed with double-row suture anchor fixation [12]. Fractures with poor bone quality and instability can be managed with the isolated conjoint tendon transfer or iliac crest bone grafting technique [13, 14]. In our study, we performed a novel double sling technique to address conjoint tendon avulsion fracture of the coracoid graft using the double sling technique as described, which is comparable to knotless bony bankart fixation. We were able to get a good bony integration of the bone block with maintained sling action of the conjoint tendon with our technique. The triple effect of the Latarjet surgery was important in maintaining the stability of the shoulder. Flow chart for Latarjet surgery coracoid graft fracture management is shown in (Chart 1).
Latarjet procedure provides good results in patients with glenohumeral instability with glenoid bone loss. The arthroscopic Laterjet technique has a steep learning curve and has the advantage of minimally invasive and fast recovery. Complication rates are almost similar to open Latarjet. Graft fractures after Latarjet procedures have been described intraoperatively. Following graft fracture, the salvage procedure depends on fracture fragment size, location of fracture, and graft stability.
This case report is to highlight the management of intraoperative coracoid graft management while performing arthroscopic Latarjet procedure. The sling effect of the conjoint tendon can be maintained with double sling fixation.
References
- 1.Dauzère F, Faraud A, Lebon J, Faruch M, Mansat P, Bonnevialle N. Is the latarjet procedure risky? Analysis of complications and learning curve. Knee Surg Sports Traumatol Arthrosc 2016;24:557-63. [Google Scholar]
- 2.Shah AA, Butler RB, Romanowski J, Goel D, Karadagli D, Warner JJ. Short-term complications of the latarjet procedure. J Bone Joint Surg Am 2012;94:495-501. [Google Scholar]
- 3.Young DC, Rockwood CA Jr. Complications of a failed Bristow procedure and their management. J Bone Joint Surg Am 1991;73:969-81. [Google Scholar]
- 4.Athwal GS, Meislin R, Getz C, Weinstein D, Favorito P. Short-term complications of the arthroscopic latarjet procedure: A North American experience. Arthroscopy 2016;32:1965-70. [Google Scholar]
- 5.Lafosse L, Boyle S. Arthroscopic latarjet procedure. J Shoulder Elbow Surg 2010;19:2-12. [Google Scholar]
- 6.Meraner D, Smolen D, Sternberg C, Thallinger C, Hahne J, Leuzinger J. 10 years of arthroscopic latarjet procedure: Outcome and complications. Indian J Orthop 2019;53:102-10. [Google Scholar]
- 7.Pereira AC, Gutierres M. Complications of coracoid transfer procedures for the treatment of recurrent shoulder dislocation. Porto Biomed J 2017;2:161-6. [Google Scholar]
- 8.Ogawa K, Inokuchi W, Matsumura N. Physeal injuries of the coracoid process are closely associated with sports activities: A systematic review. Orthop J Sports Med 2020;8:2325967120967914. [Google Scholar]
- 9.Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17-9. [Google Scholar]
- 10.Di Giacomo G, Costantini A, de Gasperis N, De Vita A, Lin BK, Francone M, et al. Coracoid bone graft osteolysis after Latarjet procedure: A comparison study between two screws standard technique vs mini-plate fixation. Int J Shoulder Surg 2013;7:1-6. [Google Scholar]
- 11.Schroder DT, Provencher MT, Mologne TS, Muldoon MP, Cox JS. The modified bristow procedure for anterior shoulder instability: 26-year outcomes in naval academy midshipmen. Am J Sports Med 2006;34:778-86. [Google Scholar]
- 12.Kongmalai P, Levine WN. Double-row fixation of the transferred coracoid process: A rescue technique for intraoperative coracoid fracture during the latarjet procedure. J Shoulder Elbow Surg 2019;28:e226-31. [Google Scholar]
- 13.Tennent D, Colaço HB, Arnander M, Pearse E. Arthroscopic conjoint tendon transfer: A technique for revision anterior shoulder stabilization. Arthrosc Tech 2016;5:e201-5. [Google Scholar]
- 14.Malahias MA, Chytas D, Raoulis V, Chronopoulos E, Brilakis E, Antonogiannakis E. Iliac crest bone grafting for the management of anterior shoulder instability in patients with glenoid bone loss: A systematic review of contemporary literature. Sports Med Open 2020;6:12. [Google Scholar]







