
Early diagnosis and management of paralabral cyst to prevent neurological deficit.
Dr. Abhishek K Gol, Trinity Hospital, Nana Mauva Main Road, Rajkot, Gujarat 360005, India. E-mail: abhishekkgol@gmail.com
Introduction: Paralabral cyst is benign fluid-filled lesion that occurs adjacent to glenoid labrum. Origin of the cyst can be traumatic or atraumatic. This cystic lesion can compress nearby axillary nerve or suprascapular nerve, resulting in shoulder pain and numbness. In this case report, we will discuss about anteroinferior paralabral cyst with axillary neuropathy in atraumatic condition.
Case Report: A 35-year-old male was admitted in our institute with complaining of numbness in the mid-part of the lateral arm and pain in the posterior aspect in the left shoulder for 2 weeks. The patient has on-and-off pain in the left shoulder on lifting weight. He had no history of trauma. X-ray was normal. On examination, tenderness presents over the dorsal aspect of shoulder and reduced sensations over deltoid muscle (regimen badge sign). Deltoid atrophy was noted. Range of motion was normal. On examination, cervical spine was normal, and reduced sensation over the lateral aspect of arm and deltoid atrophy was present. Magnetic resonance imaging (MRI) shows large multiloculated paralabral cyst caudal to inferior glenoid rim. The diagnosis was compressive axillary neuropathy which was confirmed by nerve condition study.
Conclusion: According to this case report, accurate early clinical examination and MRI evaluation are crucial in patients with atraumatic shoulder pain associated with neurological symptoms. On identification, cyst can be successfully decompressed by shoulder arthroscopy which can prevent axillary nerve damage, muscle denervation, and also recurrence of cyst can be avoided.
Keywords: Labral cyst, axillary nerve cyst decompression, hook electrode.
Paralabral cyst is very uncommon condition in adults [1]. The incidence is very low in general population [2]. The site of occurrence is more common in posterior labrum and anterior labrum, and less common in superior labrum and in inferior labrum [3]. Cause of cyst can be traumatic or atraumatic [4]. This cystic lesion can compress nearby axillary nerve or suprascapular nerve, resulting in shoulder pain and numbness [5, 6]. In this case report, we will discuss about anteroinferior paralabral cyst with axillary neuropathy in atraumatic condition. Shoulder arthroscopy was performed with cyst decompression. Paralabral cysts are a rare entity. When this condition is associated with axillary neuropathy, decompression of cyst is required to prevent axillary nerve damage and muscle denervation.
A 35-year-old male was admitted in our institute with complaining of numbness in the mid-part of the lateral arm and pain in the posterior aspect in the left shoulder for 2 weeks. The patient has on-and-off pain in the left shoulder on lifting weight. He had no history of trauma. X-ray was normal. On examination, tenderness presents over the dorsal aspect of shoulder and reduced sensations over deltoid muscle (regimen badge sign). Deltoid atrophy was noted (Fig. 1). Range of motion was normal (Fig. 2).
Range of motion was normal (Fig. 2). On examination, cervical spine was normal, and reduced sensation over the lateral aspect of arm and deltoid atrophy was present. X-ray was normal (Fig. 3).
On examination, cervical spine was normal, and reduced sensation over the lateral aspect of arm and deltoid atrophy was present. X-ray was normal (Fig. 3). Magnetic resonance imaging (MRI) shows large paralabral cyst caudal to inferior glenoid rim (Fig. 4).
Magnetic resonance imaging (MRI) shows large paralabral cyst caudal to inferior glenoid rim (Fig. 4). 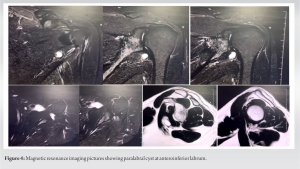 The diagnosis is compressive axillary neuropathy which was confirmed by nerve condition study. From inferior glenoid, distance of axillary nerve is around 1 cm.
The diagnosis is compressive axillary neuropathy which was confirmed by nerve condition study. From inferior glenoid, distance of axillary nerve is around 1 cm.
Surgical procedure
The patient was placed in lateral decubitus position under general anesthesia and brachial block. Diagnostic arthroscopy was done using standard posterior and anterior portals and accessory posteroinferior portal. The elevation of suspected labrum was done. Capsulotomy and cyst decompression were done using hook electrode by gradually separating structures nearby cyst. Axillary nerve exploration was done gently (Fig. 5).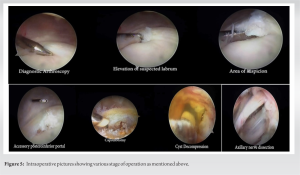
Post-operative rehabilitation
Post-operative period was uneventful. Active and passive gentle shoulder rehabilitation exercise started gradually. The patient had relief in shoulder pain after surgery. Deltoid strengthening exercise was started. 12-month postoperatively, the patient had no symptoms and Grade 5 power in deltoid muscle.
Paralabral cyst is benign fluid-filled lesion that occurs adjacent to glenoid labrum. Inferior paralabral cysts are uncommon and usually associated with labrum tear [7]. Ramaswamy et al. reported an unusual case of anteroinferior paralabral cyst with axillary nerve compression in young male with a history of fall at residence. There was a history of trauma. The patient was operated by cyst decompression and labral repair [8]. Park et al. reported Compressive Partial Neuropathy of Axillary Nerve Resulting from Anteroinferior Paralabral Cyst in an Adolescent Overhead Athlete without a history of trauma. In this case along with cyst decompression, labrum repair was done [9]. While in our case, there is no history of trauma and labrum was essentially normal. Hence, only decompression of cyst was done without labrum repair [10]. Frequency of paralabral cyst in decreasing order is anterior, posterior, superior, and inferior. Thus, inferior paralabral cysts are a rare entity. When this condition is associated with axillary neuropathy, decompression of cyst is required to prevent axillary nerve damage and muscle denervation. In this case report, the patient had atraumatic paralabral cyst associated with intact labrum. MRI and nerve condition study as well as clinical examination is crucial for diagnosis and treatment protocols.
According to this case report, accurate early clinical examination and MRI evaluation are crucial in patients with atraumatic shoulder pain associated with neurological symptoms. On identification, cyst can be successfully decompressed by shoulder arthroscopy which can prevent axillary nerve damage, muscle denervation, and also recurrence of cyst can be avoided.
Paralabral cyst can compress axillary nerve or suprascapular nerve. Clinical diagnosis can be made by EMG-NCV which can be supported with MRI picture. Although paralabral cyst is rare condition, proper evaluation is must to prevent further damage to nerve and muscle denervation.
References
- 1.Klumpp R, Gallinari G, Compagnoni R, Trevisan C. Antero-inferior paralabral cyst of the shoulder: An atypical cause of rapidly evolving axillary and musculocutaneous nerve palsy. J Clin Orthop Trauma 2020;11:S681-3. [Google Scholar]
- 2.Gartsman GM. Shoulder Arthroscopy. 2nd ed. Philadelphia, PA: WB Saunders; 2008. [Google Scholar]
- 3.Westerheide KJ, Dopirak RM, Karzel RP, Snyder SJ. Suprascapular nerve palsy secondary to spinoglenoid cysts: Results of arthroscopic treatment. Arthroscopy 2006;22:721-7. [Google Scholar]
- 4.Iannotti JP, Ramsey ML. Arthroscopic decompression of a ganglion cyst causing suprascapular nerve compression. Arthroscopy 1996;12:739-45. [Google Scholar]
- 5.Lee BC, Yegappan M, Thiagarajan P. Suprascapular nerve neuropathy secondary to spinoglenoid notch ganglion cyst: Case reports and review of literature. Ann Acad Med Singap 2007;36:1032-5. [Google Scholar]
- 6.Schroder CP, Skare O, Stiris M, Gjengedal E, Uppheim G, Brox JI. Treatment of labral tears with associated spinoglenoid cysts without cyst decompression. J Bone Joint Surg Am 2008;90:523-30. [Google Scholar]
- 7.Jeong JJ, Panchal K, Park SE, Kim YY, Lee JM, Lee JK, et al. Outcome after arthroscopic decompression of inferior labral cysts combined with labral repair. Arthroscopy 2015;31:1060-8. [Google Scholar]
- 8.Ramaswamy AG, Patil NP, Srinivasan N. An unusual case of anteroinferior paralabral cyst with axillary nerve compression: A case report. J Arthrosc Surg Sports Med 2022;3:50-2. [Google Scholar]
- 9.Park JY, Jeon SH, Oh KS, Chung SW, Lim JJ, Bang J. Compressive partial neuropathy of axillary nerve resulting from antero-inferior paralabral cyst in an adolescent overhead athlete. Korean J Sports Med 2015;33:34-39 [Google Scholar]
- 10.Dietz SO, Lichtenberg S, Habermeyer P. Non-traumatic shoulder instability in an athletic patient with a periglenoidal cyst and a glenoid labral tear. Acta Orthop Belg 2003;69:373-6. [Google Scholar]







