In the case of a hemophilic patient, surgical management is necessary and medical treatment alone is not sufficient.
Dr. Dukan Ruben, Hand, Upper Limb and Peripheral Nerve Surgery, Georges-Pompidou European Hospital (HEGP), Paris, France. E-mail: ruben.dukan@aphp.fr
Introduction: Digital artery aneurysms are a rare event but cases have been reported in the literature. The hemostasis disorders make these aneurysms particularly dangerous with potentially irreversible hand complications: Compression of adjacent vascular and nervous structures, embolization of associated thrombi, finger ischemia, and necrosis.
Case Report: We reported a case of digital ischemia due to a ruptured aneurysm of a digital collateral artery, leading to the diagnosis of congenital hemophilia A. Hematoma evacuation allowed finger revascularization. Complete symptom resolution required ligature excision associated with Factor VIII supplementation.
Conclusion: Aneurysms of the digital collateral arteries are a rare event. In the case of a hemophilic patient, surgical management is necessary, and medical treatment alone is not sufficient. The consequences of a ruptured aneurysm in this type of patient can be serious. A close monitoring is required to ensure the absence of early recurrence.
Keywords: Hemophilia, digital aneurysm, ischemia
Digital artery aneurysms are a rare event and cases have been reported in the literature [1]. Most of these aneurysms were pseudoaneurysms, corresponding to perforation of the arteria wall, related to direct blunt trauma (wound or vascular procedure) or repeated microtrauma. The hemostasis disorders make these aneurysms particularly dangerous with potentially irreversible hand complications: Compression of adjacent vascular and nervous structures, embolization of associated thrombi, finger ischemia, and necrosis. Several authors in the literature reported the management of these lesions by aneurysm excision and ligation in the majority of cases versus excision and grafting/direct suture [2-8]. In case of associated hemophilia, surgical management is usually associated with coagulation factor deficiency supplementation [9]. None of the authors reported any initial or post-operative complication in the hand. The diagnosis of hemophilia was known preoperatively. We reported the case of a patient with a pseudoaneurysm of a digital collateral artery complicated by acute ischemia due to aneurysm rupture that lead to diagnosis of hemophilia. The patient gave his consent for the publication of this clinical case.
A 36-year-old man, right-handed, non-smoker, sportive, manual worker, and without any medical background, presented with a stab wound of the left index in palmar zone 2 International Federation of Societies for Surgery of the Hand Classification [10]. Surgical procedure reported an opening of the flexor sheath without tendon injury and a continuous digital radial collateral artery with no active bleeding. After 13-day interval, the patient presented with scar swelling for 2 days. On clinical examination, vital signs were normal, without fever. There was a hypoesthesia of the radial fingertip. Palpation showed a non-compressible, pulseless but inflammatory mass. We hypothesized a surgical site infection with abscessed collection. An ultrasound assessment was performed and reported a cystic mass without any sign of blood flow inside. A surgical revision was performed. An aneurysm of the digital radial collateral artery with compression of the radial collateral nerve was identified (Fig. 1). A clamping test was performed using a clamp on the digital radial collateral artery. The finger remained vascularized on the digital ulnar collateral artery. A ligation-excision of the aneurysm was performed. Anatomopathological analysis concluded to a false aneurysm. Bacteriological examination was negative. Sensitivity of the radial fingertip was recovered immediately after surgery. After a 15-day interval, the patient presented with intense pain (visual analog scale [VAS] 8/10) in the finger with anesthesia of the radial fingertip and reappearance of a mass at the level of the scar in less than a day. An upper limb computed tomography (CT) angio was performed in emergency and showed the presence of an aneurysm below the previous ligation excision (Fig. 2).
A clamping test was performed using a clamp on the digital radial collateral artery. The finger remained vascularized on the digital ulnar collateral artery. A ligation-excision of the aneurysm was performed. Anatomopathological analysis concluded to a false aneurysm. Bacteriological examination was negative. Sensitivity of the radial fingertip was recovered immediately after surgery. After a 15-day interval, the patient presented with intense pain (visual analog scale [VAS] 8/10) in the finger with anesthesia of the radial fingertip and reappearance of a mass at the level of the scar in less than a day. An upper limb computed tomography (CT) angio was performed in emergency and showed the presence of an aneurysm below the previous ligation excision (Fig. 2).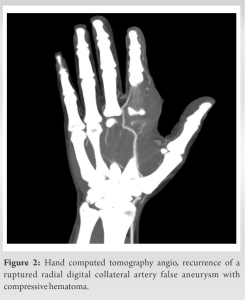 VAS was suddenly at 10/10. Clinical examination revealed acute ischemia of the finger. An emergency revision was performed. We noticed a ruptured aneurysm extending to the origin of the digital radial collateral artery from the common digital artery 1–2. Evacuation of the hematoma allowed immediate revascularization of the finger. The aneurysm was excised, and ligation was made. Sensory recovery was immediate postoperatively. Due to the recurrence, the patient was referred to the department of hematology and vascular medicine. The imaging assessment (CT angio) did not show any other aneurysmal lesions. The patient had no previous bleeding history. There was no family history of bleeding or thrombosis. The bleeding assessment tool (BAT comprises 14 categories for assessing bleeding symptoms retrospectively and it has been shown that a high bleeding score is associated with the presence of an inherited bleeding disorder) score was 4 (A score ≥4 is considered “abnormal”) and the partial thromboplastin time (PTT) ratio was 1.46 (corresponding to an intrinsic coagulation pathway defect, and thus elevated PTT). Endogenous factors were investigated and a minor factor VIII (FVIII) deficiency of 20% was found. The diagnosis of minor hemophilia A was made. A protocol of supplementation was performed: Immediately 3000 IU of FVIII and then 2000 IU every 8 h until FVIII value correction. Supplementation of FVIII deficiency and the specialized management allowed hemostasis and avoidance of early aneurysm recurrence. The patient recovered full hand function at 2 weeks postoperatively. At 1 year, we did not observe any aneurysm recurrence.
VAS was suddenly at 10/10. Clinical examination revealed acute ischemia of the finger. An emergency revision was performed. We noticed a ruptured aneurysm extending to the origin of the digital radial collateral artery from the common digital artery 1–2. Evacuation of the hematoma allowed immediate revascularization of the finger. The aneurysm was excised, and ligation was made. Sensory recovery was immediate postoperatively. Due to the recurrence, the patient was referred to the department of hematology and vascular medicine. The imaging assessment (CT angio) did not show any other aneurysmal lesions. The patient had no previous bleeding history. There was no family history of bleeding or thrombosis. The bleeding assessment tool (BAT comprises 14 categories for assessing bleeding symptoms retrospectively and it has been shown that a high bleeding score is associated with the presence of an inherited bleeding disorder) score was 4 (A score ≥4 is considered “abnormal”) and the partial thromboplastin time (PTT) ratio was 1.46 (corresponding to an intrinsic coagulation pathway defect, and thus elevated PTT). Endogenous factors were investigated and a minor factor VIII (FVIII) deficiency of 20% was found. The diagnosis of minor hemophilia A was made. A protocol of supplementation was performed: Immediately 3000 IU of FVIII and then 2000 IU every 8 h until FVIII value correction. Supplementation of FVIII deficiency and the specialized management allowed hemostasis and avoidance of early aneurysm recurrence. The patient recovered full hand function at 2 weeks postoperatively. At 1 year, we did not observe any aneurysm recurrence.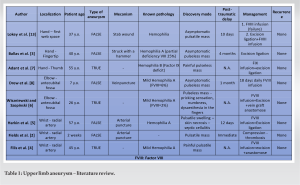
We reported a rare case of acute finger ischemia by compression of the intact digital collateral artery following a rupture of a digital collateral artery aneurysm resulting in the diagnosis of minor hemophilia A. Hemophilia is an X-linked disorder due to clotting factor VIII deficiency. Congenital hemophilia A is not known to be associated with arterial aneurysms. However, these lesions can be particularly dangerous in the hand with the risk of ischemia and necrosis of the finger in case of rupture as we have reported. We believed that the heavy bleeding of hemophilia causes extended intimal lesions with a perivascular hematoma in continuity with the vessel lumen, and pseudocavity surrounded by the adventitia, perivascular tissue, and fibrotic tissue originating from the hematoma as explained by Mann [11]. This is why we observed in our patient the aneurysm several days after the initial intimal injury. Various authors in the literature agree that hemophilia constitutes an excess risk in case of aneurysm [3, 7, 12]. The chronology of our case report is consistent with the various cases in the literature on post-traumatic hand pseudoaneurysm [3, 13]. There is an intimal lesion that will progressively dissect due to the continuous bleeding. This kind of complication must be differentiated from the risk of embolization of arterial aneurysms that can also lead to digital ischemia [4]. We can consider this risk to be lower in the hemophilia patient. To date, the prevalence of pseudoaneurysms in patients with hemophilia is not known and the optimal strategy has yet to be defined. Although Drew et al. [8] suggested that factor replacement was an adequate option in healthy hemophilia patients without inhibitors when pseudoaneurysms are small, we believe that these patients should be systematically managed with either excision/ligation or direct suture/grafting, considering the risk of acute ischemia by rupture and compression. Given the extensive intimal lesions that we have reported, we believe that the ligation solution is the safest strategy to avoid the development of an aneurysm proximal to the graft. It is obvious that in case of insufficient vascularization by a single artery, an anastomose with graft is required [3]. Lokey et al. [13] reported a case of failure of medical treatment, alone with continuous aneurysm growth until rupture and the need for emergency hemostasis and ligation. A blood hemostasis test is required in case of digital aneurysm (true or pseudo aneurysm). The resolution of the symptoms in our case was only observed after FVIII supplementation. Elective surgical repair under proper FVIII concentrate infusion is safe, whereas surgery in an emergency setting may be hazardous for the patient. In the upper limb, cases of aneurysm are sporadic, and it is not possible to know their frequency (Table 1). The main difference with our case is the absence of a diagnosis of hemophilia at the time of management, except for the case reported by Fields concerning a 2-month-old child [2].
Aneurysms of the digital collateral arteries are a rare event. In the case of a hemophilic patient, surgical management is necessary and medical treatment alone is not sufficient. The consequences of a ruptured aneurysm in this type of patient can be fatal. A close monitoring is required to ensure the absence of early recurrence.
Digital aneurysm is a rare event. Patient should be screened for hemophilia. Medical treatment is a mandatory complement to surgery to avoid recurrence.
References
- 1.Sheikh Z, Selvakumar S, Goon P. True aneurysm of the digital artery: A case report and systematic literature review. J Surg Case Rep 2020;2020:rjz400. [Google Scholar]
- 2.Fields JM, Saluja S, Schwartz DS, Touloukian RJ, Keller MS. Hemophilia presenting in an infant as a radial artery pseudoaneurysm following arterial puncture. Pediatr Radiol 1997;27:763-4. [Google Scholar]
- 3.Ballas KD, Rafailidis SE, Kouskouras KA, Fardellas J, Alatsakis MB, Sakadamis AK. False aneurysm of the proper palmar digital artery--report of a case. Acta Chir Belg 2006;106:249-51. [Google Scholar]
- 4.Filis K, Arhontovassilis F, Theodorou D, Theodossiades G, Manouras A. True radial artery aneurysm in a mild haemophilia A patient. Haemophilia 2007;13:440-2. [Google Scholar]
- 5.Harkin DW, Connolly D, Chandrasekar R, Anderson M, Blair PH, Hood JM, et al. Radial artery mycotic pseudoaneurysm in a haemophiliac: A potentially fatal complication of arterial catheterization. Haemophilia 2002;8:721-4. [Google Scholar]
- 6.Wiszniewski A, Szopiński P. Surgical treatment of arteriovenous fistula and brachial artery aneurysm in a patient with mild haemophilia A. Haemophilia 2011;17:548-50. [Google Scholar]
- 7.Adant JP, Grattagliano B, Fissette J. True aneurysm of digital artery in hemophilia. A case report. Ann Chir Main Memb Super 1994;13:278-81. [Google Scholar]
- 8.Drew M, Yu JC, Michaels LA. Arterial pseudoaneurysms in haemophilia: Conservative treatment with observation and factor replacement. Haemophilia 2011;17:550-2. [Google Scholar]
- 9.Diplaris KT, Karfis EA, Ampatzidou F, Ananiadou OG, Vakalopoulou S, Madesis A, et al. Acute type-a dissection in a patient with severe hemophilia A. J Cardiothorac Vasc Anesth 2012;26:660-3. [Google Scholar]
- 10.Castel LC, Hurst SA, Masmejean E, Gregory TM. Hand wounds: An analysis of topography and related damage to underlying structures. Injury 2022;53:4048-53. [Google Scholar]
- 11.Mann HA, Goddard NJ, Lee CA, Brown SA. Periarticular aneurysm following total knee replacement in hemophilic arthropathy. A case report. J Bone Joint Surg Am 2003;85:2437-40. [Google Scholar]
- 12.Sleightholm R, Wahlmeier S, Carson JS, Drincic A, Lazenby A, Foster JM. Massive adrenal vein aneurysm mimicking an adrenal tumor in a patient with hemophilia A: A case report and review of the literature. J Med Case Rep 2016;10:343. [Google Scholar]
- 13.Lokey H, Phelps DB, Boswick JA. Traumatic false aneurysm of the hand in hemophilia. J Trauma 1978;18:283-4. [Google Scholar]