
Orthopedic surgeons should be cautious about complications of broken guide wire during hip fracture surgeries and when encountered, it should be retrieved through lesser morbid options before resorting to an open approach through the pelvis.
Dr. Ashraf Shaikh, Department of Orthopaedics, 6th Floor New Building, Seth G.S. Medical College and King Edward VII Memorial Hospital, Acharya Donde Marg, Parel East, Mumbai - 40 0012, Maharashtra, India. E-mail: ashrafshaikh123@gmail.com
Introduction: Hardware breakage during surgery is a known risk that may result in serious complications. Drill bits and guide wires are particularly prone to breakage, and if not promptly recognized and removed, can cause damage to intrapelvic structures, or may lead to hip arthritis later. Herein, we present two cases in which broken guide wire fragments were safely retrieved through the same incision, resulting in good outcomes and reduced morbidity.
Case Report: In the first case, a broken guide wire piece that had been pushed into the hip joint during intertrochanteric fracture surgery was retrieved using disc forceps after reaming over the same guide tract. In the second case, the broken tip of a partially withdrawn guide wire was removed from a transcervical femur fracture using a cannulated drill bit.
Conclusion: Our approach highlights the importance of attempting retrieval of broken hardware through the same tract using unconventional instruments, such as disc forceps, before resorting to more invasive methods, such as arthrotomy or separate incisions. These cases demonstrate the feasibility of this approach and its potential to reduce morbidity associated with hardware retrieval.
Keywords: Proximal femur fracture, broken hardware, unconventional methods, drill bits, guide wires, disc forceps.
The breakage of orthopedic hardware is rare during surgical management of proximal femur fractures. Drill bits and guide wires are the most common hardware that breaks during surgery. Broken pieces within the femur can sometimes be left in place without any suspected complications. Rarely, a broken guide wire can extend into the hip joint or migrate partially or completely into the pelvis. These require surgical removal as the broken wire may lead to hip arthritis or cause trauma to intrapelvic structures such as the external iliac vein or pelvic viscera. We report two cases in which the guide wire broke intraoperatively within the femur, and we managed to retrieve it through the same incision, thus reducing morbidity and achieving good outcomes.
Case 1
A 52-year-old man presented to the emergency room with an Evans type 2 intertrochanteric hip fracture. Proximal femoral nailing with a proximal femoral nail antirotation II (PFN A2) implant was planned. Under spinal anesthesia, closed reduction was achieved on a fracture table in the supine position. The guide wire was inserted from the tip of the greater trochanter (GT) using a skin incision 7 cm proximal to the GT. An appropriately sized nail was inserted after proximal reaming. A 3 mm guide wire was then used to insert the helical blade from the lateral cortex to the femoral head. However, while inserting the helical blade, it was observed that a broken piece of the guide wire had been pushed into the hip joint and pelvis with the blade still midway in its tract (Fig. 1a). Various options for the retrieval of the broken guide wire were discussed immediately. The helical blade and nail were removed, and the blade tract was manually followed with a size 8 tibia reamer up to the distal tip of the broken guide wire. Under fluoroscopic guidance, a disc forceps was used to retrieve the free end of the broken piece. The fracture was then ultimately fixed with a dynamic hip screw system (Fig. 1b). The post-operative course was uneventful, and the patient recovered well.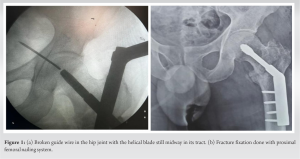
Case 2
A 42-year-old man was admitted with a transcervical neck of femur fracture. A percutaneous three-screw fixation was planned. Under spinal anesthesia, closed reduction was achieved on a fracture table in the supine position. A 1.8 mm guide wire was passed in the calcar region using a power drill. However, due to the inaccurate trajectory of the guide wire, it was planned to withdraw the wire using a drill gun. While removing it, a sudden giveaway was felt and we realized that the tip of the partially withdrawn wire broke. Fluoroscopy revealed the broken guide wire in the subcapital region of the neck, reaching the head without any intra-articular extension (Fig. 2a). To retrieve the broken piece, a 4.5 mm cannulated drill bit was used on a drill gun and advanced over half of the extent of the broken wire under fluoroscopic guidance (Fig. 2a). The broken wire got engaged within the drill bit and was successfully retrieved on withdrawing the drill bit. The fracture was then managed as planned with a three-screw fixation and the recovery was uneventful (Fig. 2b).
Drill bits followed by guide wires are the most common orthopedic hardware that breaks intraoperatively [1, 2]. Literature-recorded techniques for addressing a broken guide pin involve the use of either an intraosseous route through the femur or a separate open approach. Over-reaming of the guide tract and use of long, small bore retrieval forceps is a well-documented technique owing to its simplicity [3, 4]. Arthroscopically assisted methods, although minimally invasive, are not readily available, expensive, and have a long learning curve.  The use of intraosseous “bone endoscopy” using the tract made for the blade, to extract the broken piece endoscopically was successfully used by Arora et al. [5]. Both of our cases were middle-aged men with considerable cancellous bone quality which may be responsible for the breakage of the guide pin under resistance offered by the strong bone interface. We believe that the chances of such events occurring are less when dealing with osteoporotic or poor bone quality. One must keep this in mind while dealing with hip surgeries that involve good bone quality and not force their way or hammer the wire/pin/drill bit through the tough cancellous bone. Another possible cause may be the use of an old guide pin or a wire that has previously been used multiple times. Breakage is common while using such wires and the risk of failure is when the screw is being inserted over the wire or a tract is being drilled [6]. Stakeholders must ensure regular replacement of these wires from the implant set. A particular concern while using PFN A2 implant is the hammering of a larger bore blade over an un-reamed smaller guide pin tract as it is expected to gain better purchase when compared with manual screwing of the blade [7]. While this may hold true for an osteoporotic bone, hammering over a smaller bore guide wire in a good-quality cancellous bone may evoke stresses in the guide pin if there is a mismatch in the tracts of the pin and the blade. This we believe was the cause of breakage in the first case. Similarly, forceful progression of a sub-optimally sharp guide pin with a drill gun in a good-quality cancellous bone may bend the guide pin, disobeying a linear path. When this guide pin is withdrawn it fails to contour to the curvilinear trajectory and breaks midway. This was observed in the second case scenario. In both cases, we managed to remove the broken wire safely avoiding arthrotomy or any other approach. Previously (6) authors have successfully retrieved intraarticular broken hardware using surgical approaches such as which can increase the morbidity of the patient Salunke et al. [1] However if the broken wire migrates into the pelvis, possible options include laparoscopic retrieval [8] or laparotomy with an extraperitoneal ilioinguinal approach [9] which may require the expertise of other surgeons. In the first case, we had to remove the in situ nail owing to the nail hindering the path of exploration into the femur head. A similar method was used by Garabadi and O’Brien which needed implant removal and reimplantation [4]. Krishna and Chand used a technique involving a manually controlled drill bit on a T handle with sequential drilling of bone just distal to the broken wire with repetitive cleaning of bone debris from the drill bit and using a Kerrison rongeur to retrieve the piece [3]. They were able to achieve this without needing implant removal reducing operative time and maintaining fixation. The relatively non-invasive methods have certain drawbacks, first, the use of reamers to enlarge the tract for retrieval with disc forceps causes bone stock loss in the femoral head. Multiple attempts may cause considerable bone loss compromising the hold of the implant needed for fixation of fractures of the proximal femur. There is a considerable risk of pushing the broken pin further in the pelvis by the approaching reamer/drill bit abutting the piece (11). There have been records of neurovascular injuries such as injury to the external iliac vein from broken pins/wires that migrated into the pelvis [10]. This complication must be kept in mind while removing the broken guide wire. The use of an image intensifier in two orthogonal planes during the advancement of the reamer/drill bit can reduce the chances of it.
The use of intraosseous “bone endoscopy” using the tract made for the blade, to extract the broken piece endoscopically was successfully used by Arora et al. [5]. Both of our cases were middle-aged men with considerable cancellous bone quality which may be responsible for the breakage of the guide pin under resistance offered by the strong bone interface. We believe that the chances of such events occurring are less when dealing with osteoporotic or poor bone quality. One must keep this in mind while dealing with hip surgeries that involve good bone quality and not force their way or hammer the wire/pin/drill bit through the tough cancellous bone. Another possible cause may be the use of an old guide pin or a wire that has previously been used multiple times. Breakage is common while using such wires and the risk of failure is when the screw is being inserted over the wire or a tract is being drilled [6]. Stakeholders must ensure regular replacement of these wires from the implant set. A particular concern while using PFN A2 implant is the hammering of a larger bore blade over an un-reamed smaller guide pin tract as it is expected to gain better purchase when compared with manual screwing of the blade [7]. While this may hold true for an osteoporotic bone, hammering over a smaller bore guide wire in a good-quality cancellous bone may evoke stresses in the guide pin if there is a mismatch in the tracts of the pin and the blade. This we believe was the cause of breakage in the first case. Similarly, forceful progression of a sub-optimally sharp guide pin with a drill gun in a good-quality cancellous bone may bend the guide pin, disobeying a linear path. When this guide pin is withdrawn it fails to contour to the curvilinear trajectory and breaks midway. This was observed in the second case scenario. In both cases, we managed to remove the broken wire safely avoiding arthrotomy or any other approach. Previously (6) authors have successfully retrieved intraarticular broken hardware using surgical approaches such as which can increase the morbidity of the patient Salunke et al. [1] However if the broken wire migrates into the pelvis, possible options include laparoscopic retrieval [8] or laparotomy with an extraperitoneal ilioinguinal approach [9] which may require the expertise of other surgeons. In the first case, we had to remove the in situ nail owing to the nail hindering the path of exploration into the femur head. A similar method was used by Garabadi and O’Brien which needed implant removal and reimplantation [4]. Krishna and Chand used a technique involving a manually controlled drill bit on a T handle with sequential drilling of bone just distal to the broken wire with repetitive cleaning of bone debris from the drill bit and using a Kerrison rongeur to retrieve the piece [3]. They were able to achieve this without needing implant removal reducing operative time and maintaining fixation. The relatively non-invasive methods have certain drawbacks, first, the use of reamers to enlarge the tract for retrieval with disc forceps causes bone stock loss in the femoral head. Multiple attempts may cause considerable bone loss compromising the hold of the implant needed for fixation of fractures of the proximal femur. There is a considerable risk of pushing the broken pin further in the pelvis by the approaching reamer/drill bit abutting the piece (11). There have been records of neurovascular injuries such as injury to the external iliac vein from broken pins/wires that migrated into the pelvis [10]. This complication must be kept in mind while removing the broken guide wire. The use of an image intensifier in two orthogonal planes during the advancement of the reamer/drill bit can reduce the chances of it.
Guide wire breakage can be a sudden and dreaded intraoperative complication during hip fracture surgery. Attempts must be made to retrieve it through the same tract using unconventional instruments such as disc forceps before employing a more invasive separate incision approach.
Orthopedic surgeons must be aware of the possibility of guide wire breakage during hip surgeries and must keep instruments that can be used for wire retrieval as standby for the same. An attempt of less invasive retrieval must be made as the step of choice.
References
- 1.Salunke AA, Menon PH, Nambi GI, Tan J, Patel V. Removing a broken guidewire in the hip joint: Treatment options and recommendations for preventing an avoidable surgical catastrophe. A case report. Sao Paulo Med J 2015;133:531-4. [Google Scholar]
- 2.Sen RK, Tripathy SK, Aggarwal S, Agarwal A, Goyal T, Tahasildar N, et al. Broken Kirschner or guide-wire retrieval: A report of 4 cases. Hip Int 2010;20:551-4. [Google Scholar]
- 3.Krishna D, Chand S. A simple technique to retrieve broken guide wire transfixing hip joint. J Orthop Allied Sci 2015;3:31. [Google Scholar]
- 4.Garabadi M, O’Brien S. Broken guidewire retrieval from the hip joint: A case report. Trauma Case Rep 2021;35:100512. [Google Scholar]
- 5.Arora S, Maini L, Aggarwal V, Dhal A. Broken guidewire protruding into the hip joint: A bone endoscopic-assisted retrieval method. Indian J Orthop 2012;46:109-12. [Google Scholar]
- 6.Price MV, Molloy S, Sollan MC, Sutton A, Ricketts DM. The rate of instrument breakage during orthopaedic procedures. Int Orthop 2002;26:185-7. [Google Scholar]
- 7.Gadhe DS, Bhor DP, Patel DI, Vatkar DA, Kale DS, Kanade DG. Comparative study of PFNA versus pfna 2 in unstable intertrochanteric fractures: A randomised control study of 50 cases. Int J Orthop Sci 2019;5:162-4. [Google Scholar]
- 8.Kottmeier S, Born CT, Saul H. Laparoscopic retrieval of a migrating intrapelvic pin: Case report and review of literature. J Trauma 1993;35:952-5. [Google Scholar]
- 9.Afshar A. Intrapelvic protrusion of a broken guide wire fragment during fixation of a femoral neck fracture. Arch Bone Joint Surg 2017;5:63-5. [Google Scholar]
- 10.Siegel A, Schulz F, Püschel K. Fatal injury to the external iliac vein by a guide wire during use of a dynamic hip screw (DHS). Unfallchirurg 2001;104:182-6. [Google Scholar]
- 11.Peivandi MT, Kachooei AR, Nazemian Z. New method to remove a broken guide pin in the hip joint. Orthopedics 2011;34:e685-7. [Google Scholar]








