
Complications related to Subtrochanteric Osteotomy for neglected Developmental Dysplasia of Hip can be avoided with staged Total Hip Arthroplasty.
Dr. Praveen Kumar Anbalagan, Department of Orthopaedics, MGM Medical College, Navi Mumbai - 410 209, Maharashtra, India. E-mail: drpraveen93@yahoo.com
Introduction: Developmental dysplasia of hip (DDH) is an abnormal development of hip joint which when neglected in early age group can lead to joint pain and secondary osteoarthritic changes. Crowe types III and IV neglected DDH joint is widely managed with total hip arthroplasty with subtrochanteric shortening.
Case Report: A 52-year-old female presented with neglected DDH joint which was managed in two stages with femoral lowering followed by uncemented total hip arthroplasty without osteotomy.
Conclusion: With the two-stage procedure, subtrochanteric shortening which is widely accepted management for neglected DDH and the related complications were avoidable with a satisfactory Harris hip score.
Keywords: Developmental dysplasia of hip, arthroplasty, subtrochanteric osteotomy.
Developmental dysplasia of hip (DDH) constitutes a group of anatomic hip abnormalities that influence the development and stability of the hip during the early growth period. The reported incidence of DDH varies from 1.5 to 2.5/1000 live births [1, 2]. Patients with DDH when left untreated may eventually develop secondary osteoarthritis and present during the middle age. The underlying pathology is unique and presents structural features that need to be addressed in the course of treatment. Crowe classification is the most widely used methods to classify the hip dysplasia, which compared the level of extent of femoral head to the height of the normal femoral head or pelvis. According to the classification, the present case is a Crowe type III DDH [3]. Total hip arthroplasty is one of the most accepted methods to treat secondary osteoarthritis in adult with neglected DDH with or without subtrochanteric shortening depending upon the migration of the head from the true acetabulum. It is commonly believed that DDH is accompanied with acetabular deficiency more on the lateral and anterior wall, with excessive ante version. The deformities associated with femur include excessive ante version, a displaced greater trochanter, increased neck-shaft angle, underdeveloped medullary canal, rotational metaphyseal-diaphyseal malalignment, and abductor muscles contracture [4]. Therefore, total hip replacement in DDH in adult age group requires prior detailed planning. We present a case of a 52-year-old female with left hip osteoarthritis secondary to DDH managed with two staged progressive femoral lowering followed by uncemented total hip arthroplasty.
A 52-year-old female homemaker presented with difficulty in walking since childhood and pain in left hip which aggravated for the past 2–3 years. The patient had a painful limp on presentation. The pain was insidious in onset, gradually progressive, dull aching type, with no diurnal variation, aggravated on movements and walking for long duration and partly relieved on rest. There was deep tenderness on the greater trochanter which was broadened and thickened. Thomas test and Trendelenburg test were positive. There were adduction of 10°, abduction of 40°, and rotations of 5° each. There was fixed flexion deformity of 10° with a further flexion of 80° possible with limb length discrepancy of 4 cm. Anteroposterior pelvis with hips radiographs and computerized tomography scan confirmed a left-sided hypoplastic bony anatomy characterized by shallow acetabula, insufficient coverage of the femoral head, deficient anterior acetabular wall, and excessive anteversion (Fig. 1).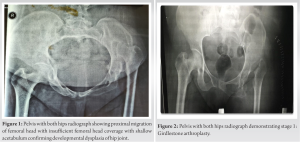 After thorough discussion with the patient and planning, two staged procedure was planned. In the first stage, a Girdlestone excision arthroplasty with posterior approach, adductor tenotomy was performed, globular soft-tissue release along with adhesions was done, true and false acetabulum were visualized (Fig. 2). The patient was then kept on a skeletal traction with weight increments (up to 15 kg) for a period of 3 weeks, and about 3 cm of femur lowering was achieved at the end of 3 weeks clinically (Fig. 3).
After thorough discussion with the patient and planning, two staged procedure was planned. In the first stage, a Girdlestone excision arthroplasty with posterior approach, adductor tenotomy was performed, globular soft-tissue release along with adhesions was done, true and false acetabulum were visualized (Fig. 2). The patient was then kept on a skeletal traction with weight increments (up to 15 kg) for a period of 3 weeks, and about 3 cm of femur lowering was achieved at the end of 3 weeks clinically (Fig. 3).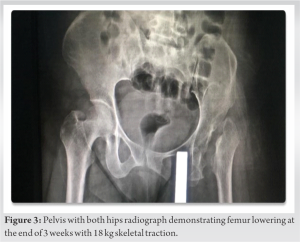 During this period of bed rest with skeletal traction, the patient was managed with antibiotics and deep vein thrombosis prophylaxis preoperative sizing of the acetabular cup and femoral head with the help of 3D-printed pelvis (Fig. 4) was achieved and in the second stage, an uncemented total hip was performed using posterior approach performed (Fig. 5) (acetabular cup 42 mm, femoral head 22 mm with 2-mm neck length, femoral stem 85 mm, screw 20 mm × 6.5 mm, and screw 25 mm × 6.5 mm).
During this period of bed rest with skeletal traction, the patient was managed with antibiotics and deep vein thrombosis prophylaxis preoperative sizing of the acetabular cup and femoral head with the help of 3D-printed pelvis (Fig. 4) was achieved and in the second stage, an uncemented total hip was performed using posterior approach performed (Fig. 5) (acetabular cup 42 mm, femoral head 22 mm with 2-mm neck length, femoral stem 85 mm, screw 20 mm × 6.5 mm, and screw 25 mm × 6.5 mm). 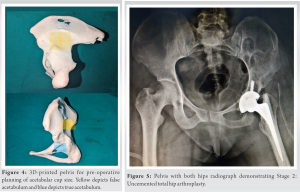 Physiotherapy was started the following day and full weight bearing with crutches was started on day 2 of post-operative period. The patient achieved 100° of hip flexion with knees flexed, 20° of extension, and 20° of abduction; walks comfortably with mild quadriceps lag at 2-year follow-up; and was evaluated with Harris hip score.
Physiotherapy was started the following day and full weight bearing with crutches was started on day 2 of post-operative period. The patient achieved 100° of hip flexion with knees flexed, 20° of extension, and 20° of abduction; walks comfortably with mild quadriceps lag at 2-year follow-up; and was evaluated with Harris hip score.
There are several critical issues to be dealt with while planning a total hip arthroplasty in a Crowe types 3 or 4 DDH for better long-lasting results. The common surgical difficulties faced are total capsulectomy, acetabular placement, anatomical restoration of hip center, and subtrochanteric shortening. Acetabular cup placement is desirable to be placed at the true acetabulum in an attempt to restore the normal center of hip rotation and optimal abductor muscle function. However, Murayama et al. [5] in a study concluded that Harris hip score was better achieved with high cup placement compared to Harris hip score of patients with anatomical true cup placement but found higher polyethylene wear rates in high cup placement group compared to group with anatomical true cup placement. Cemented acetabular components along with autogenous bone graft showed favorable outcomes but mid-term results showed graft collapse particularly when the acetabulum has been filled with large amount of cancellous bone and the cup is cemented without pressure [6]. Uncemented acetabular components showed favorable outcomes. In the present case, we used uncemented acetabular cup which showed good outcome at 2-year follow-up. There are no definitive guidelines in terms of acceptable lengthening, excessive lengthening may cause sciatic nerve palsy, and the present case achieved 2 cm lengthening on the operated side which was negated with a show raise. Subtrochanteric shortening with total hip arthroplasty is widely accepted surgical line of management for reconstruction in neglected DDH joint. However, subtrochanteric shortening-related documented complications include nonunion, delayed union, cement interposition at the subtrochanteric osteotomy site [7, 8, 9], and nerve palsy. To avoid these complications, Binazzi et al. [10] performed total hip replacement in twelve patients with neglected DDH without subtrochanteric osteotomy and observed good Harris hip score. In this study, the authors performed the procedure in two stages, in the first stage, the progressive femoral lowering was performed with external fixator compared to skeletal traction as used in the current case report and after achieving the required length, total hip replacement was performed. Binazzi et al. [10] in this cohort study used external fixator for progressive lowering of the femur wherein two or three pins are driven into the iliac bone above the acetabulum which was later modified with moving the external fixator more distally to avoid infection around the operative site and distally into the supracondylar region. In our case report, the progressive femur lowering was achieved with distal femur pin with weight increments over 3 weeks and after the desired length was achieved, total hip arthroplasty was performed without the need for subtrochanteric shortening and related complications. At the final follow-up, the patient was evaluated with Harris hip score, which was 84 at 2-year follow-up. Despite the above modifications from the widely accepted line of management, the only limitation in the proposed management of progressive femur lowering with skeletal traction is the prolonged hospital stay and time period between the two procedures.
Total hip arthroplasty with subtrochanteric shortening is considered to be gold standard for Crowe types III and IV DDH. However, the following procedures documented complications such as nerve palsy, cement interposition at the osteotomy site, non-union, and malunion. The staged femoral lowering followed by cementless total hip arthroplasty provided satisfactory outcome in 52-year-old female.
Total hip arthroplasty in DDH can be managed with femoral lowering avoiding the complications related to subtrochanteric shortening.
References
- 1.Suzuki S, Seto Y, Futami T, Kashiwagi N. Preliminary traction and the use of under-thigh pillows to prevent avascular necrosis of the femoral head in pavlik harness treatment of developmental dysplasia of the hip. J Orthop Sci 2000;5:540-5. [Google Scholar]
- 2.Gustke K. Hip pathologies that bedevil the dysplastic hip. Bone Joint J 2013;95-B:31-6. [Google Scholar]
- 3.Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am 1979;61:15-23. [Google Scholar]
- 4.Wang Y. Current concepts in developmental dysplasia of the hip and Total hip arthroplasty. Arthroplasty 2019;1:2. [Google Scholar]
- 5.Murayama T, Ohnishi H, Okabe S, Tsurukami H, Mori T, Nakura N, et al. 15-year comparison of cementless total hip arthroplasty with anatomical or high cup placement for Crowe I to III hip dysplasia. Orthopedics 2012;35:e313-8. [Google Scholar]
- 6.Busch VJ, Clement ND, Mayer PF, Breusch SJ, Howie CR. High survivorship of cemented sockets with roof graft for severe acetabular dysplasia. Clin Orthop Relat Res 2012;470:3032-40. [Google Scholar]
- 7.Charity JA, Tsiridis E, Sheeraz A, Howell JR, Hubble MJ, Timperley AJ, et al. Treatment of Crowe IV high hip dysplasia with total hip replacement using the exeter stem and shortening derotational subtrochanteric osteotomy. J Bone Joint Surg Br 2011;93:34-8. [Google Scholar]
- 8.Hasegawa Y, Iwase T, Kanoh T, Seki T, Matsuoka A. Total hip arthroplasty for Crowe Type IV developmental dysplasia. J Arthroplasty 2012;27:1629. [Google Scholar]
- 9.Kerboull M, Hamadouche M, Kerboull L. Total hip arthroplasty for Crowe Type IV developmental hip dysplasia: A long-term follow-up study. J Arthroplasty 2001;16:170-6. [Google Scholar]
- 10.Binazzi R. Two-stage progressive femoral lowering followed by cementless total hip arthroplasty for treating Crowe IV-hartofilakidis Type 3 developmental dysplasia of the hip. J Arthroplasty 2015;30:790-6. [Google Scholar]






