
Unusual cause of EHL tendon rupture repaired using novel turndown flap technique providing tension-free repair.
Dr. Rohan, Junior Clinical Fellow, Department of Trauma and Orthopaedics, Wythenshawe Hospital (Manchester University NHS Foundation Trust) Southmoor Road, Manchester, M23 9LT, United Kingdom. E-mail: rohan7@doctors.net.uk
Introduction: We present a case of spontaneous rupture of the extensor hallucis longus (EHL) tendon with significantly retracted tendon edges in a patient who had received multiple steroid injections to an arthritic talonavicular joint repaired using novel turndown flap technique.
Case Report: This case details a patient who came in with a history of spontaneous EHL tendon rupture on a background of chronic pain in the midfoot due to osteoarthritis with osteophytes at the talonavicular joint for which they had received multiple steroid injections in the past. A novel repair technique was employed which involved split lengthening the proximal segment of the ruptured EHL tendon and making a turndown flap of the same by rotating the lengthened segment 180°, bridging the tendon gap. The lengthened tendon is then sutured to the distal segment of the EHL to achieve a tension-free repair. This bypasses any use of bridging allografts and autografts/tendon transfer, removing complications commonly associated with them.
Conclusion: This turndown flap technique is easy to perform, reduces surgical time, avoids complications associated with tendon grafting, and results in good functional outcomes for the patient.
Keywords: Extensor hallucis longus tendon rupture, turndown flap, steroid injection.
We present a case of spontaneous rupture of the extensor hallucis longus (EHL) tendon in a patient who had received multiple steroid injections to an arthritic talonavicular joint. EHL tendon injuries commonly occur due to lacerations to the dorsum of the foot [1]. Spontaneous EHL tendon injuries are a rare phenomenon. However, the literature links such injuries with certain medical conditions, namely diabetes mellitus [2], obesity [2], local steroid injections [2, 3], and osteophytes [4].
We reviewed a 43-year-old female patient reporting spontaneous onset of sharp pain around the left midfoot with subsequent difficulty in extending the great toe for the past 12 months. She had a history of chronic pain in the midfoot due to osteoarthritis with osteophyte at the talonavicular joint for which she had received multiple steroid injections. Her examination revealed tenderness and a palpable osteophyte at the talonavicular joint. In addition, active extension of the big toe was weak compared to the opposite foot. She was, however, able to bear weight and walk with some discomfort. An MR scan (Fig. 1) confirmed the EHL tendon rupture with a retracted proximal end lying at the level of the tibiotalar joint. To address this issue, she was taken up for open surgical repair using a longitudinal incision over the dorsum of the foot exposing the EHL tendon. The tendon edges had retracted with a 5 cm gap between them (Fig. 2).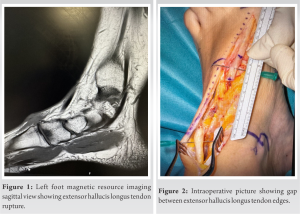 The proximal stump was identified at the level of the ankle joint and the distal stump at the talonavicular joint. The tendon edges were debrided and repaired using a turndown flap technique. The proximal stump was divided along its thickness to lift a flap measuring around 5 cm (Fig. 3). The turndown flap was used to bridge the gap between tendon edges and sutured to the distal stump (Fig. 4).
The proximal stump was identified at the level of the ankle joint and the distal stump at the talonavicular joint. The tendon edges were debrided and repaired using a turndown flap technique. The proximal stump was divided along its thickness to lift a flap measuring around 5 cm (Fig. 3). The turndown flap was used to bridge the gap between tendon edges and sutured to the distal stump (Fig. 4). Kirschner wire (K-wire) was used to stabilize the first metatarsophalangeal joint in extension (Fig. 5), and a below knee plaster cast was applied. K-wires were removed at 6 weeks. However, a slipper cast was maintained for immobilization for 9 weeks, after which weight bearing was commenced in a walking boot. She began a range of motion exercises under the supervision of a physiotherapist from 12th week onward. In her latest clinic review, the patient’s pain had entirely resolved, she could actively dorsiflex the great toe, and her Foot and Ankle Ability Measure score had significantly improved from 18/84 pre-operatively to 64/84.
Kirschner wire (K-wire) was used to stabilize the first metatarsophalangeal joint in extension (Fig. 5), and a below knee plaster cast was applied. K-wires were removed at 6 weeks. However, a slipper cast was maintained for immobilization for 9 weeks, after which weight bearing was commenced in a walking boot. She began a range of motion exercises under the supervision of a physiotherapist from 12th week onward. In her latest clinic review, the patient’s pain had entirely resolved, she could actively dorsiflex the great toe, and her Foot and Ankle Ability Measure score had significantly improved from 18/84 pre-operatively to 64/84.
EHL is a muscle of the anterior compartment of the leg responsible for the extension of the hallux, dorsiflexion of the foot at the ankle, and inversion of the foot [5]. During the gait cycle, the heel is the first point of contact with the ground, after which the ground reaction forces apply a plantar flexion moment to the foot. Dorsiflexors of the foot resist this and help to gradually lower the rest of the foot to come in contact with the ground. EHL deficiency will render the medial side of the foot weak and unable to control this descent toward the ground. The absence of EHL function can also lead to curling of the big toe while wearing a shoe and tripping while walking. We believe that repairing the torn EHL tendon improves gait and function. However, literature evidence for the management of this injury is contentious. For example, Griffiths [6], in his series of patients with tendon injuries around the ankle, had concluded that formal repair of the EHL tendon was unnecessary due to its natural tendency to repair spontaneously after tenotomy. However, five of the six patients in his series with EHL rupture had undergone surgical repair to obtain a satisfactory outcome. Contrarily, Wong et al. [7] concluded that surgical repair or reconstruction is a reliable procedure to restore alignment and function in their retrospective review of 23 patients with EHL tendon rupture. They advocate acute repair if tendon edges can be approximated without tension and suggest grafting/tendon transfer when there is a gap. However, we observe that even a gap of up to 5 cm can be repaired tension free with this novel turndown flap technique. The turndown flap technique has been previously described in Achilles tendon repair [8]. It involves split lengthening the proximal segment and rotating it by 180° to bridge the gap before suturing it onto the distal stump. Joseph and Barhorst [9] used a similar technique to repair EHL laceration by split lengthening the distal stump. We have instead used the proximal stump for split lengthening, which enables us to bridge wider gaps, as evidenced in this case report. Tendon grafting, in the form of either allografting or autografting, is another viable option to bridge gaps and ensure tension-free repair. However, allografting is limited in availability and involves higher costs and risks such as infection and rejection [1]. Alternatively, autografts of semitendinosus [10], gracilis [11], extensor digitorum longus [7, 12], palmaris longus [13], plantaris, and peroneus tertius [14] can be used to avoid complications associated with allografting but they still carry risks such as donor site morbidity and increased surgical time. A turndown flap technique avoids all the above-mentioned complications altogether. As regards to post-operative management, there is a dearth of literature to guide us regarding mobilization protocol after such a tendon repair. Therefore, we favored caution by protecting the repair for 12 weeks to minimize the risk of tendon re-rupture before the patient started physiotherapy.
We present a novel turndown flap technique of EHL tendon rupture management with this case report which can bridge significant gaps, 5 cm in this case, between the tendon ends along with providing a tension-free repair. This turndown flap technique is easy to perform, reduces surgical time, avoids complications associated with tendon grafting, and results in good functional outcomes for the patient.
This case report aims to highlight the need for judicious use of steroid injections in osteoarthritis keeping in mind its associated complications as well as presenting a novel turndown flap technique for EHL tendon repair.
References
- 1.Bastías GF, Cuchacovich N, Schiff A, Carcuro G, Pellegrini MJ. Technique tip: EDL-to-EHL double loop transfer for extensor hallucis longus reconstruction. Foot Ankle Surg 2017;25:272-7. [Google Scholar]
- 2.Holmes GB Jr., Mann RA. Possible epidemiological factors associated with rupture of the posterior tibial tendon. Foot Ankle 1992;13:70-9. [Google Scholar]
- 3.Ford LT, DeBender J. Tendon rupture after local steroid injection. South Med J 1979;72:827-30. [Google Scholar]
- 4.Fadel GE, Alipour F. Rupture of the extensor hallucis longus tendon caused by talar neck osteophyte. Foot Ankle Surg 2008;14:100-2. [Google Scholar]
- 5.Lezak B, Summers S. Anatomy, bony pelvis and lower limb: Extensor hallucis longus muscle. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022-2023. [Google Scholar]
- 6.Griffiths JC. Tendon injuries around the ankle. J Bone Joint Surg Br 1965;47:686-9. [Google Scholar]
- 7.Wong JC, Daniel JN, Raikin SM. Repair of acute extensor hallucis longus tendon injuries: A retrospective review. Foot Ankle Spec 2013;7:45-51. [Google Scholar]
- 8.Ponnapula P, Aaranson RR. Reconstruction of Achilles tendon rupture with combined V-Y plasty and gastrocnemius-soleus fascia turndown graft. J Foot Ankle Surg 2010;49:310-5. [Google Scholar]
- 9.Joseph RM, Barhorst J. Surgical reconstruction and mobilization therapy for a retracted extensor hallucis longus laceration and tendon defect repaired by split extensor hallucis longus tendon lengthening and dermal scaffold augmentation. J Foot Ankle Surg 2012;51:509-16. [Google Scholar]
- 10.Park HG, Lee BK, Sim JA. Autogenous graft repair using semitendinous tendon for a chronic multifocal rupture of the extensor hallucis longus tendon: A case report. Foot Ankle Int 2003;24:506-8. [Google Scholar]
- 11.Smith B, Coughlin M. Reconstruction of a chronic extensor hallucis longus tendon laceration with a Gracilis tendon autograft. Orthopedics 2008;31:(10):orthosupersite.com/view.asp?rID=31525. [Google Scholar]
- 12.Leung YF, Ip SP, Chung OM. A new method of functional tendon transfer for the dysfunction of extensor hallucis longus. Foot Ankle Int 2002;23:1124-5. [Google Scholar]
- 13.Al-Qattan MM. Surgical treatment and results in 17 cases of open lacerations of the extensor hallucis longus tendon. J Plast Reconstr Aesthet Surg 2007;60:360-7. [Google Scholar]
- 14.Coughlin MJ, Schon LC. Disorders of the tendons. In: Saltzman CL, Anderson RB, editors. Mann’s Surgery of the Foot and Ankle. 9th ed. Philadelphia, PA: Saunders/Elsevier; 2013. p. 1188-291. [Google Scholar]





