
Bilateral posteromedial tibial plateau fracture detection after low-energy trauma and appropriate surgical exposure for treatment.
Dr. Serdar Demiröz, Department of Orthopaedics and Traumatology, Kocaeli University, Izmitm, Turkey. E-mail: serdardemiroz@hotmail.com
Introduction: Tibial plateau fractures account for average 1% of all fractures in adults. They mostly related to high-energy trauma in young adult and milder traumatic injuries in elderly due to osteoporosis.
Case Report: In this case, we reported a 28-year-old male patient who admitted to the emergency room with painful and swollen bilateral knees who had fallen on his knees while playing leapfrog. When his friend jumped on his back, he fell on his knees with the forced flexion and valgus of the knee. Plain radiographs of the knees revealed bilateral posterior tibial plateau fractures. Open reduction and internal fixation were the choice of treatment. Full range of motion was allowed but not weight-bearing for 2 months. At 6 months of follow-up, the patient had full range of motion and weight-bearing with no complaint.
Conclusion: We present bilateral posteromedial tibial plateau fracture in a healthy young adult which is not mentioned in the literature before and we want to emphasize that posteromedial approach in the supine position, even for both knees in the same operation session, is appropriate to reach the fracture and reduce it easily.
Keywords: Plateau fracture, bilateral, posteromedial approach, isolated.
Tibial plateau fractures account for average 1% of all fractures in adults [1]. Because they are articular fractures, anatomical reduction and stable fixation which enable early mobilization are mandatory like all other articular fractures. They mostly related to high-energy trauma in young adult and milder traumatic injuries in elderly due to osteoporosis. About only 8% of plateau fractures occur in more than 65 years of age [2]. Many classification systems have been used in the past, and Schatzker et al. have the most widely used one today [3]. It splits the fractures into six types according to the involvement of condyles and fracture patterns. Most of the fractures are unicondylar, and the lateral plateau fractures contribute 90% of these cases. Thirty percentages to 35% of cases are bicondylar [4]. Although posterior tibial fracture fragment seen in two-thirds of bicondylar tibial plateau fractures, isolated posterior tibial plateau fracture (PTPF) is relatively uncommon with an incidence of 7.8% and it is not sufficiently included in classification systems [5, 6]. Chen et al. proposed a new classification system by classifying PTPFs into five categories. According to this classification, split fracture of posteromedial condyle consists only 18% of all PTPFs [7]. Because it is rare and mostly related to high-energy trauma like traffic accidents, we report an interesting case of bilateral isolated posteromedial tibial plateau fracture occurred during leapfrogging in a healthy young adult.
A 28-year-old male was admitted to the emergency room with painful and swollen bilateral knees who had fallen on his knees while playing leapfrog. When his friend jumped on his back, he fell on his knees with the forced flexion and valgus of the knee. On examination, there was gross sensitivity with palpation and swelling. The bilateral range of motion was painful and limited. Neurovascular examination and adjacent joints were normal. Varus and valgus stress tests could not be applied due to gross pain. Plain radiographs of the knees revealed bilateral PTPF (Fig. 1). The bone quality was good, and there is no metabolic disease or chronic drug use. A computed tomography scan was performed to clarify the fracture pattern and plan the appropriate treatment. Bilateral posteromedial displaced fracture fragment was seen easily in the 3D scan (Fig. 2).
The bone quality was good, and there is no metabolic disease or chronic drug use. A computed tomography scan was performed to clarify the fracture pattern and plan the appropriate treatment. Bilateral posteromedial displaced fracture fragment was seen easily in the 3D scan (Fig. 2).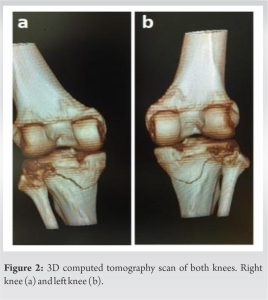 Elective surgery was planned to wait for reduction of edema. The patient was placed in supine position and bilateral knee examination was performed under general anesthesia. There was no major instability. Tourniquet was used after prophylactic antibiotic administration. The leg was abducted and externally rotated and put in a figure of 4 position, and then, posteromedial approach was performed. A straight incision was made running from the medial epicondyle to the posteromedial edge of the tibia. After opening the fascia, the fracture was reached by passing through the pes anserinus and gastrocnemius and then reduced anatomically and fixed with a plate. Then, the same procedure was applied to the other knee. Postoperatively, full range of motion was allowed but not weight-bearing for 2 months. At 6 months of follow-up, the patient had full range of motion and weight-bearing with no complaint. The patient al
Elective surgery was planned to wait for reduction of edema. The patient was placed in supine position and bilateral knee examination was performed under general anesthesia. There was no major instability. Tourniquet was used after prophylactic antibiotic administration. The leg was abducted and externally rotated and put in a figure of 4 position, and then, posteromedial approach was performed. A straight incision was made running from the medial epicondyle to the posteromedial edge of the tibia. After opening the fascia, the fracture was reached by passing through the pes anserinus and gastrocnemius and then reduced anatomically and fixed with a plate. Then, the same procedure was applied to the other knee. Postoperatively, full range of motion was allowed but not weight-bearing for 2 months. At 6 months of follow-up, the patient had full range of motion and weight-bearing with no complaint. The patient al so underwent magnetic resonance imaging scan at last follow-up and there was no major soft tissue injury.
so underwent magnetic resonance imaging scan at last follow-up and there was no major soft tissue injury.
Isolated posterior tibial fractures are rare and account for only 7.8% of all tibial plateau fractures, and then, isolated posteromedial split fracture accounts only 18% of all PTPF, so it is an extremely rare injury. In our case, we report bilateral isolated posteromedial split fracture of the tibial plateau which is not mentioned before in the literature. This is the first interest of our case. On the other hand, the tibial plateau is the most critical load bearing area in the body, and the most common mechanism of the fracture involves axial loading by femoral condyle to the tibial plateau with the varus or valgus stress when the knee is at semi-flexion. In general, it results from high-energy trauma secondary to motor vehicle accidents or a fall from a height in young patients. In this case, the injury happened such a low-energy trauma; patient fallen on his knees while playing leapfrog, in a healthy young adult, so this is the second interest of our case. Bae et al. reported an interesting case of bilateral fracture of the medial tibial plateau following a motorcycle accident in a patient who had arthroscopic anterior cruciate ligament reconstruction in the past, but isolated posteromedial tibial plateau fracture with low-energy-induced trauma in a healthy adult is not mentioned before [8]. There are controversies about the surgical approaches and fixation methods for PTPF because it is difficult to reduce and stabilize the fracture by conventional approaches and techniques. The posteromedial approach has been widely used in the treatment of posteromedial fracture, and satisfactory results have been achieved [9]. The posterior midline approach also may be suitable for fractures extend to the lateral, but it is more likely to injure popliteal vessels and tibial nerve. Due to the anatomy of the posterior tibial plateau which is transition area of the metaphysis and has a great degree of curvature, there is no available internal fixator that fits anatomically [10], so t-shaped plate or reconstruction plate is a possible choice for fixation after accurate molding. In this case, we present bilateral posteromedial tibial plateau fracture in a healthy young adult which is not mentioned in the literature before and we want to emphasize that posteromedial approach in the supine position, even for both knees in the same operation session, is appropriate to reach the fracture and reduce it easily. Then, for the fixation, we used reconstruction plate for one side and the tubular plate for another. Because, the profile of the plates should be low enough to allow bending to adopt the anatomy of posterior tibial plateau. We started to the passive range of motion exercises just after the 1st day of the operation but not weight-bearing until the fracture healing. After 6 months of follow-up, the patient had full range of motion without any complication (Fig. 3).
Bilateral posteromedial tibial plateau fracture might be seen in healthy young adults even by a low-energy trauma. Surgical treatment can be performed in supine position with posteromedial approach safe and easily in a single session.
Bilateral posteromedial tibial plateau fracture might be seen as a result of a low-energy trauma and can be managed by posteromedial approach in supine position in a single session easily.
References
- 1.Burdin G. Arthroscopic management of tibial plateau fractures: Surgical technique. Orthop Traumatol Surg Res 2013;99:S208‑18. [Google Scholar]
- 2.Hsu CJ, Chang WN, Wong CY. Surgical treatment of tibial plateau fracture in elderly patients. Arch Orthop Trauma Surg 2003;121:67-70. [Google Scholar]
- 3.Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience 1968--1975. Clin Orthop 1979;138:94-104. [Google Scholar]
- 4.Duparc J, Ficat P. Fractures articulaires de l’extrémité supérieure du tibia. Rev Chir Orthop Reparatrice Appar Mot 1960;46:399-486. [Google Scholar]
- 5.Chang SM, Zheng HP, Li HF, Jia YW, Huang YG, Wang X, et al. Treatment of isolated posterior coronal fracture of the lateral tibial plateau through posterolateral approach for direct exposure and buttress plate fixation. Arch Orthop Trauma Surg 2009;129:955-62. [Google Scholar]
- 6.Maripuri SN, Rao P, Manoj-Thomas A, Mohanty K. The classification systems for tibial plateau fractures: How reliable are they? Injury 2008;39:1216-21. [Google Scholar]
- 7.Chen HW, Chen CQ, Yi XH. Posterior tibial plateau fracture: A new treatment-oriented classification and surgical management. Int J Clin Exp Med 2015;8:472-9. [Google Scholar]
- 8.Bae KC, Cho CH, Lee KJ. Bilateral medial tibial plateau fracture after arthroscopic anterior cruciate ligament reconstruction. Knee Surg Relat Res 2015;27:129-32. [Google Scholar]
- 9.De Boeck H, Opdecam P. Posteromedial tibial plateau fractures. Operative treatment by posterior approach. Clin Orthop Relat Res 1995;320:125-8. [Google Scholar]
- 10.Chen H, Wu L. Surgical options for posterior tibial plateau fracture. Int J Clin Exp Med 2015;8:21421-7. [Google Scholar]





