The management of humeral head osteonecrosis as a complication of rotator cuff repair and the treatment with a reverse total shoulder arthroplasty.
Dr. Amir Mhiri, Department of Orthopaedic Surgery, Sahloul Hospital, 4054 Sousse, Tunisia. E-mail: amirmhiri1@gmail.com
Introduction: The osteonecrosis and the collapse of the humeral head may have many risk factors such as trauma, alcoholism, metabolic diseases, and corticosteroid therapy. Otherwise, it was described as a rare complication of shoulder arthroscopy in the past few years.
Case Report: We report the case of a 65-year-old right-handed woman who had a rotator cuff tear of the right shoulder. She underwent a double-row arthroscopic repair. Six months later she had an intense shoulder pain, with radiological and MRI signs of humeral head osteonecrosis. The patient had a reverse total shoulder arthroplasty.
Conclusion: The aim of this case report is to underline the diagnostic particularities of this complication, and to shed light on the pathogenesis of the interruption of blood supply in the humeral head following rotator cuff repair. We also discuss the management of this complication with reverse total shoulder arthroplasty.
Keywords: Shoulder, rotator cuff, arthroscopy, humeral head, osteonecrosis.
Rotator cuff tears are a common pathology in the elderly, causing invalid pain and shoulder disability [1]. The surgical treatment consists in arthroscopic repair of the torn tendons using suture anchors. This treatment option has good outcomes with some complications such as infection, delayed wound healing, algodystrophy, stiffness, and deep venous thrombosis [2]. Osteonecrosis of the humeral head is a rare cause of shoulder pain. It has many traumatic and metabolic etiologies [3]. The disruption of the vascular supply of the humeral head was the common factor [4]. A few cases described this osteonecrosis as a complication of shoulder arthroscopy with a rapid progressive severe pain and collapse of the humeral head within the 1st year following surgery [5, 6, 7]. In this report, we aim to describe this rare complication and to provide more information about the risk factors and the treatment options.
A 65-year-old, right-hand dominant woman, presented with 1-year history of rotator cuff syndrome of the right shoulder. Plain radiographs showed a maintained acromiohumeral distance with no signs of osteoarthritis (Fig. 1).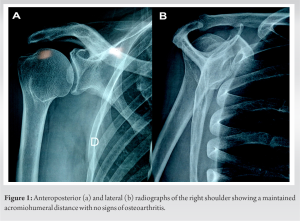 Magnetic resonance imaging (MRI) showed full-thickness tear of the supraspinatus muscle with Goutallier Stage 1 fatty degeneration, normal signals of the humeral head and the glenoid cavity were observed (Fig. 2).
Magnetic resonance imaging (MRI) showed full-thickness tear of the supraspinatus muscle with Goutallier Stage 1 fatty degeneration, normal signals of the humeral head and the glenoid cavity were observed (Fig. 2).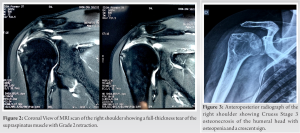 The patient underwent shoulder arthroscopy that confirmed the full-thickness tears of the supraspinatus with Patte Type 2 retraction. We performed a double-row repair for the tendon using two suture anchors. Concomitant biceps tenotomy and acromioplasty were also performed. The patient was allowed to do self-assisted passive motion in the first 4 weeks postoperatively. Full active motion was initiated 6 weeks after the surgery then muscle strengthening physical therapy was prescribed 2 weeks later. At 3-month follow-up, the patient had a good range of motion in all planes without any complications. Six months postoperatively, the patient presented with severe right shoulder pain and restriction of all ranges of motion. Physical examination found tenderness around the anterior aspect of the shoulder with only 30° of forward elevation and abduction. The white blood cell count and the C-reactive protein level were within the normal limits. Shoulder radiographs revealed Cruess Stage 3 osteonecrosis of the humeral head with osteopenia and a crescent sign (Fig. 3 and 4).
The patient underwent shoulder arthroscopy that confirmed the full-thickness tears of the supraspinatus with Patte Type 2 retraction. We performed a double-row repair for the tendon using two suture anchors. Concomitant biceps tenotomy and acromioplasty were also performed. The patient was allowed to do self-assisted passive motion in the first 4 weeks postoperatively. Full active motion was initiated 6 weeks after the surgery then muscle strengthening physical therapy was prescribed 2 weeks later. At 3-month follow-up, the patient had a good range of motion in all planes without any complications. Six months postoperatively, the patient presented with severe right shoulder pain and restriction of all ranges of motion. Physical examination found tenderness around the anterior aspect of the shoulder with only 30° of forward elevation and abduction. The white blood cell count and the C-reactive protein level were within the normal limits. Shoulder radiographs revealed Cruess Stage 3 osteonecrosis of the humeral head with osteopenia and a crescent sign (Fig. 3 and 4). 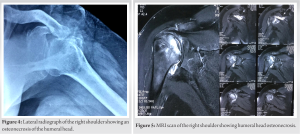 MRI was consistent with humeral head osteonecrosis (Fig. 5). Due to the severe pain and the disability, the patient was treated with a reverse total shoulder arthroplasty 2 months after the diagnosis of osteonecrosis (Fig. 6).
MRI was consistent with humeral head osteonecrosis (Fig. 5). Due to the severe pain and the disability, the patient was treated with a reverse total shoulder arthroplasty 2 months after the diagnosis of osteonecrosis (Fig. 6).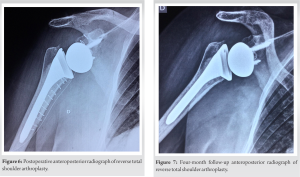 At the 4-month follow-up, the shoulder was not painful with an acceptable range of motion. The patient had 90° of abduction, 100° of forward elevation and she was highly satisfied with the outcome (Fig. 7).
At the 4-month follow-up, the shoulder was not painful with an acceptable range of motion. The patient had 90° of abduction, 100° of forward elevation and she was highly satisfied with the outcome (Fig. 7).
Shoulder arthroscopy may have some complications such as infection, neurovascular injuries, stiffness, algodystrophy, and even deep venous thrombosis leading to death. These complications can occur in 5.8%–10.6% of cases [2]. Osteonecrosis of the humeral head can have many non-traumatic causes, with the interruption of the blood supply as a common point [4]. These non-traumatic etiologies include corticosteroid therapy, alcoholism, Gaucher’s disease, dysbarism, and pregnancy [3]. The understanding of vascular anatomy and its variations is crucial for surgeons before proximal humerus procedures or shoulder arthroscopy [8]. The pathogenesis of humeral head osteonecrosis after shoulder arthroscopy was referred by some authors to a perioperative injury of the anterolateral branch of the anterior circumflex humeral artery by a poor placement of suture anchor or the use of multiple anchors [7]. However, Dilisio et al. [6] could not conclude that aberrant use of suture anchors was linked to the osteonecrosis because no hardware was used in two of the three patients in their study. Other suggested that additional damage might occur at the level of the biceps tenotomy or tenodesis [9]. In fact, the anterior circumflex humeral artery and its anterolateral branch may present anatomical variations leading to a higher risk of injury during biceps tenodesis tenotomy or placement of suture anchors [10]. Therefore, post-arthroscopic humeral head osteonecrosis can result from a damage to the anterolateral branch at the level of the transverse humeral ligament and the biceps tendon, or a damage to the intraosseous blood supply in the great tubercle, or both concurrently [10]. However, the poor intraosseous blood supply of the superomedial aspect of the humeral head makes it the initial starting location of osteonecrosis [9, 10]. The coagulation of blood vessels using radiofrequency, the increasing pressure and temperature of intra-articular fluid, embolism, and prolonged traction seem to be involved in the mechanisms of osteonecrosis. Possible allergic reactions or hypersensitivity due to the bioabsorbable suture anchors can also be involved in combination with the other mentioned factors [11]. Due to the severe pain and the disability, reverse total shoulder arthroplasty was the treatment of choice in many reported cases, with satisfying functional results [11].
The knowledge of the anatomy of humeral head vascularization is necessary for shoulder surgeons, in a way to avoid this rare complication. Variations of the anterior circumflex humeral artery and its anterolateral branch should be taken in consideration. Thus, humeral head osteonecrosis leads to inevitable reinterventions for shoulder arthroplasty which can be risky in elderly patients with comorbidities. Further studies are required to establish a clear relationship between shoulder arthroscopy and rapid progressive osteonecrosis of the humeral head.
To underline the diagnostic particularities of humeral head osteonecrosis following a rotator cuff repair using an anchor, and to shed light on the pathogenesis of the interruption of blood supply in the humeral head following rotator cuff repair.
References
- 1.Moosmayer S, Smith HJ, Tariq R, Larmo A. Prevalence and characteristics of asymptomatic tears of the rotator cuff: An ultrasonographic and clinical study. J Bone Joint Surg Br 2009;91:196-200. [Google Scholar]
- 2.Brislin KJ, Field LD, Savoie FH 3rd. Complications after arthroscopic rotator cuff repair. Arthroscopy 2007;23:124-8. [Google Scholar]
- 3.Hasan SS, Romeo AA. Nontraumatic osteonecrosis of the humeral head. J Shoulder Elbow Surg 2002;11:281-98. [Google Scholar]
- 4.Harreld KL, Marker DR, Wiesler ER, Shafiq B, Mont MA. Osteonecrosis of the humeral head. J Am Acad Orthop Surg 2009;17:345-55. [Google Scholar]
- 5.Beauthier V, Sanghavi S, Roulot E, Hardy P. Humeral head osteonecrosis following arthroscopic rotator cuff repair. Knee Surg Sports Traumatol Arthrosc 2010;18:1432-4. [Google Scholar]
- 6.Dilisio MF, Noble JS, Bell RH, Noel CR. Postarthroscopic humeral head osteonecrosis treated with reverse total shoulder arthroplasty. Orthopedics 2013;36:e377-80. [Google Scholar]
- 7.Goto M, Gotoh M, Mitsui Y, Okawa T, Higuchi F, Nagata K. Rapid collapse of the humeral head after arthroscopic rotator cuff repair. Knee Surg Sports Traumatol Arthrosc 2015;23:514-6. [Google Scholar]
- 8.Fontes EB, Precht BL, Andrade RC, Fernandes RM, Cisne R. Output relations of humeral circumflex arteries and its variations. Int J Morphol 2015;33:1171-5. [Google Scholar]
- 9.Keough N, de Beer T, Uys A, Hohmann E. An anatomical investigation into the blood supply of the proximal humerus: Surgical considerations for rotator cuff repair. JSES Open Access 2019;3:320-7. [Google Scholar]
- 10.Keough N, Lorke DE. The humeral head: A review of the blood supply and possible link to osteonecrosis following rotator cuff repair. J Anat 2021;239:973-82. [Google Scholar]
- 11.Kim JK, Jeong HJ, Shin SJ, Yoo JC, Rhie TY, Park KJ, et al. Rapid progressive osteonecrosis of the humeral head after arthroscopic rotator cuff surgery. Arthroscopy 2018;34:41-7. [Google Scholar]