
Total elbow arthroplasty is still relevant today, even in younger population giving good functional outcomes.
Dr. Aniket Wagh, Department of Orthopaedics, Employees’ State Insurance Hospital, Kandivali, Mumbai, India. E-mail: ani4u8725@gmail.com
Introduction: Certain elbow pathologies can give rise to considerable loss of joint function, which would severely affect the daily living activities of the patients. Total elbow arthroplasty (TEA) can be a safe and reasonable motion-preserving and pain-relieving option in such debilitating elbow conditions. The aim of this case series is to evaluate the functional outcome of TEA in young patients with four different indications after an 8-year follow-up.
Case Report: We report a case series of four TEA cases done for different indications, namely rheumatoid arthritis, chronic elbow dislocation, post-traumatic elbow ankylosis, and failed primary total elbow replacement, all in relatively young patients. All patients were given a semi-constrained Coonrad-Morrey prosthesis using a posterior Bryan–Morrey approach. The cases were done during the years 2013–2014. Eight-year follow-up of each case showed excellent functional outcome and persistent pain relief with a high Mayo Elbow Performance Score. All the patients have given written consent for publishing this article.
Conclusion: Despite being uncommon, total elbow replacement can be the choice of surgery for certain elbow affections, giving satisfactory functional recovery and good pain relief, even in a younger population.
Keywords: Total elbow arthroplasty, replacement, elbow, rheumatoid arthritis, mayo elbow performance score.
The elbow being one of the most mobile joints, its smooth and complete range of movement (ROM) is necessary for the good functioning of the upper extremity. The elbow has a normal movement range of full extension to 145° of flexion and about 160° of prono-supination [1]. Within this range, an individual requires at least 30–130° of flexion and rotation between 50° of supination and 50° of pronation for average daily activities [2]. Dee described total elbow arthroplasty (TEA) for the 1st time in 1972 to treat patients with RA. However, there have been constant modifications in the techniques and implant designs of TEA [3], which has led to the realization that its indications could include complex comminuted elbow fractures, post-traumatic arthrosis and ankylosis, chronic instability, failure of fracture fixation, and even elbow osteoarthritis [4-10]. Elbow prosthesis has undergone rapid evolution and refinement since it was first described. At present, the available prostheses are of the following types:
Unconstrained
Ewald’s capitello-condylar design is an example. Since components here are unlinked, it requires functional collateral ligaments and a good soft tissue envelope. It would also ideally require good bone quality. The most common complication reported is instability. (5–10% dislocation) [11]. Thus, the component alignment needs to be perfect.
Semiconstrained
It has a sloppy hinge that gives some rotational and varus-valgus freedom, thus reducing stress on the bone-cement interface and the incidence of component loosening. It has the best results of all the designs. The radial head need not be replaced. The anterior flange of the humeral component resists posteriorly directed and rotational forces. The Coonrad-Morrey design is an example [11].
Constrained
Constrained is considered to be the most stable type. It has a rigidly hinged design. Highest loosening rate amongst the three. Dee’s design is an example of a constrained elbow prosthesis [11].
Case 1
39-year-old female with right elbow stiffness and non-relieving pain due to rheumatoid arthritis (RA). The movement arc was only 20° (80–100° of flexion). Eight years post-operatively she had excellent ROM and good pain relief, with a Mayo Elbow Performance Score (MEPS) of 85.
Case 2
A 48-year-old female with chronic untreated right elbow dislocation since childhood resulting in an ankylosed joint with only jog of movements possible. Eight years post-op, painless and near-complete ROM with MEPS of 100.
Case 3
A 26-year-old male with a completely ankylosed elbow at 90° due to a year-old history of a compound comminuted fracture of the right proximal ulna, which was fixed followed by implant removal. Excellent functional results 8 years post-operatively with MEPS of 100.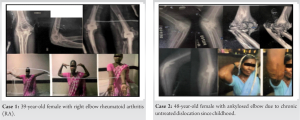
Case 4
A 35-year-old female with right TEA done 2 years ago presented with a broken prosthesis hinge, resulting in multiaxial elbow instability. Revision surgery was done. Intra-op, the broken screw of the hinge could not be retrieved due to excessive fibrosis. Ulna was fractured during the removal of the cement mantle, which was fixed with wires. We managed to get a good functional ROM post-operatively and MEPS of 85 at 8-year follow-up.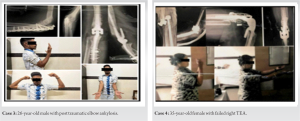
Operative technique
All surgeries were performed by the same surgeon. A semi-constrained Coonrad-Morrey prosthesis by ZIMMER was used in all four cases. Surgeries were performed with the patient in a supine position with the forearm supported on the torso (Fig. 1). The posterior Bryan-Morrey approach was used (Fig. 2). 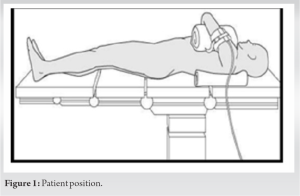 The average operative time was 118 minutes. Care was taken to isolate and protect the ulnar nerve (Fig. 3).
The average operative time was 118 minutes. Care was taken to isolate and protect the ulnar nerve (Fig. 3).  The olecranon process was preserved to provide a good lever arm for the triceps to work on. To improve flexion and extension, anterior capsulotomy and triceps release were done, respectively. The flexor muscles were released if found contracted. After preparing the ulna and humerus canals, reduction was done with trial components (Fig. 4 and 5), followed by definitive cemented component implantation (Fig. 6). Cementing was done with the help of an endotracheal tube (Fig. 7).
The olecranon process was preserved to provide a good lever arm for the triceps to work on. To improve flexion and extension, anterior capsulotomy and triceps release were done, respectively. The flexor muscles were released if found contracted. After preparing the ulna and humerus canals, reduction was done with trial components (Fig. 4 and 5), followed by definitive cemented component implantation (Fig. 6). Cementing was done with the help of an endotracheal tube (Fig. 7).  The ROM was always confirmed under anesthesia. Triceps were secured to the olecranon through drill holes. The patient was given an arm pouch post-op. X-rays were done the same day. Physiotherapy was started the very next day in the form of passive- and active-assisted elbow ROM exercises. Three doses of antibiotics were given, and the patient was discharged on the third post-op day.
The ROM was always confirmed under anesthesia. Triceps were secured to the olecranon through drill holes. The patient was given an arm pouch post-op. X-rays were done the same day. Physiotherapy was started the very next day in the form of passive- and active-assisted elbow ROM exercises. Three doses of antibiotics were given, and the patient was discharged on the third post-op day.
Follow-up
Suture removal was done after 2 weeks. At 3-month follow-up, all patients had a ROM arc of around 120° (10–130°) of flexion-extension and around 130° of prono-supination. Follow-up X-rays showed good alignment. There were no wound- or neurovascular-related problems. All patients were able to carry out their activities of daily living (ADL) with varying degrees of comfort level. All patients were followed up after 8 years to see for functional outcomes.
At 8 years of follow-up, the results were persistent, with no new complaints from any of the patients. There was no evidence of loosening, heterotrophic ossification, or osteolysis in any of the cases. All of them had excellent functional outcomes with MEPS in the range of good to excellent (85–100).
A few decades ago, it was believed that the survival rate for total elbow replacement was low. Moreover, complications like damage to the radial and ulnar nerves, periprosthetic fractures, infection, and wound dehiscence were also established [7, 12, 13]. These were a few of the main reasons against its use. Surgeons thus resorted to salvage substitutes like elbow joint fusion and soft tissue interposition arthroplasty, but they too were accused of low functional scores and a high number of drawbacks [14-18]. Using newly developed designs and techniques, TEA has now been reported to have a 5-year survival rate of 97.7% and a 10-year survival rate of 91.0% [7]. It has emerged as a viable option for end-stage elbow pathologies, even in younger patients, with favorable results. Park et al. conducted a retrospective study of 23 semi-constrained elbow arthroplasties in a younger population of <40 years, which showed a 95% rate of survival at 8 years and 89% at 15. These were surprisingly close to the survival rates of TEA in older populations [19]. In another review of the literature by Welsink et al., they studied 9379 elbow arthroplasties done for various pathologies. The mean rate of survival at 7.8 years was 85.5%, and at 12.3 years, it was 74% [20]. Celli and Morrey, in their study of 55 TEAs done in a population below 45 years of age, showed that 93%, i.e., 51 patients, had a Mayo performance score of 85 and above [21]. This has encouraged surgeons to consider TEA for various indications, even in a younger population. There are still some complications that are being reported in TEA, clinical loosening being the most frequent one [20,22,23]. Reviewing the literature points out that the lowest outcomes were seen in patients with previous elbow trauma, with higher failure and complication rates [24, 25]. The reason for this could be that post-traumatic osteoarthritis of the elbow is seen more frequently in active young patients and is associated with soft tissue contractions, fixed deformities, loose bone stock, and previously done surgeries, which would increase the complication rates [8]. In this case series, we did not encounter any of these complications except for the intra-op olecranon fracture in one case. The 8-year functional outcomes of all four cases are excellent and worth reporting.
Despite having some complications, elbow arthroplasties have stood the test of time and are in fact proving to be a good treatment choice for several elbow pathologies, including complex trauma and primary osteoarthritis. It can give good functional results, even in young patients, as we have shown in this case series, with a rapid return to performing ADL.
- TEA is a pain-relieving and motion-preserving procedure that still has its indications.
- TEA continues to provide good functional outcomes for end-stage elbow pathologies, even in a younger population.
- TEA has its own set of complications, the most common being the loosening of the prosthesis. However, they can be tackled with newer designs and better techniques.
References
- 1.Soucie JM, Wang C, Forsyth A, Funk S, Denny M, Roach K, et al. Hemophilia treatment center network. Range of motion measurements: Reference values and a database for comparison studies. Haemophilia 2011;17:500-7. [Google Scholar]
- 2.Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63:872-7. [Google Scholar]
- 3.Dee R. Total replacement arthroplasty of the elbow for rheumatoid arthritis. J Bone Joint Surg Br 1972;54:88-95. [Google Scholar]
- 4.Barco R, Streubel PN, Morrey BF, Sanchez-Sotelo J. Total elbow arthroplasty for distal humeral fractures: A ten-year-minimum follow-up study. J Bone Joint Surg Am 2017;99:1524-31. [Google Scholar]
- 5.Barthel PY, Mansat P, Sirveaux F, Dap F, Mole D, Dautel G. Is total elbow arthroplasty indicated in the treatment of traumatic sequelae? 19 cases of Coonrad-Morrey(®) reviewed at a mean follow-up of 5.2 years. Orthop Traumatol Surg Res 2014;100:113-8. [Google Scholar]
- 6.Cikes A, Jolles BM, Farron A. Open elbow arthrolysis for posttraumatic elbow stiffness. J Orthop Trauma 2006;20:405-9. [Google Scholar]
- 7.Mansat P, Bonnevialle N, Rongières M, Mansat M, Bonnevialle P. Experience with the Coonrad-Morrey total elbow arthroplasty: 78 consecutive total elbow arthroplasties reviewed with an average 5 years of follow-up. J Shoulder Elbow Surg 2013;22:1461-8. [Google Scholar]
- 8.Mansat P, Morrey BF. Semi-constrained total elbow arthroplasty for ankylosed and stiff elbows. J Bone Joint Surg Am 2000;82:1260-8. [Google Scholar]
- 9.Mansat P, Degorce HN, Bonnevialle N, Demezon H, Fabre T, SOFCOT. Total elbow arthroplasty for acute distal humeral fractures in patients over 65 years old-results of a multicenter study in 87 patients. Orthop Traumatol Surg Res 2013;99:779-84. [Google Scholar]
- 10.Plaschke HC, Thillemann TM, Brorson S, Olsen B. Implant survival after total elbow arthroplasty: A retrospective study of 324 procedures performed from 1980 to 2008. J Shoulder Elbow Surg 2014;23:829-36. [Google Scholar]
- 11.Orthobullets. Available from: https://www.orthobullets.com/shoulder-and-elbow/3089/total-elbow-arthroplasty Last accessed on 2022]. [Google Scholar]
- 12.Morrey BF. Complications of elbow replacement surgery. In: The Elbow and Its Disorders. Netherlands: Elsevier; 2000. p. 667-76. [Google Scholar]
- 13.Shi LL, Zurakowski D, Jones DG, Koris MJ, Thornhill TS. Semi-constrained primary and revision total elbow arthroplasty with use of Coonrad-Morrey prosthesis. J Bone Joint Surg Am 2007;89:1467-75. [Google Scholar]
- 14.Chen DD, Forsh DA, Hausman MR. Elbow interposition arthroplasty. Hand Clin 2011;27:187-97. [Google Scholar]
- 15.Delloye C, Cornu O, Dubuc JE, Vincent A, Barbier O. Elbow reconstruction with massive total osteoarticular allograft: Early failure due to instability. Rev Chir Orthop Reparatrice Appar Mot 2004;90:360-4. [Google Scholar]
- 16.Erşen A, Demirhan M, Atalar AC, Salduz A, Tunali O. Stiff elbow: Distraction interposition arthroplasty with an Achilles tendon allograft: Long-term radiological and functional results. Acta Orthop Traumatol Turc 2014;48:558-62. [Google Scholar]
- 17.Larson AN, Morrey BF. Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am 2008;90:2714-23. [Google Scholar]
- 18.Urbaniak JR, Black KE. Cadaveric elbow allografts. A six-year experience. Clin Orthop Relat Res 1985;197:131-40. [Google Scholar]
- 19.Park JG, Cho NS, Song JH, Lee DS, Rhee YG. Clinical outcomes of semi-constrained total elbow arthroplasty in patients who were forty years of age or younger. J Bone Joint Surg Am 2015;97:1781-91. [Google Scholar]
- 20.Welsink CL, Lambers KT, van Deurzen DF, Eygendaal D, van den B, Michel PJ. Total elbow arthroplasty: A systematic review. JBJS Rev 2017;5:e4. [Google Scholar]
- 21.Celli A, Morrey BF. Total elbow arthroplasty in patients forty years of age or less. J Bone Joint Surg Am 2009;91:1414-8. [Google Scholar]
- 22.Puskas GJ, Morrey BF, Sanchez-Sotelo J. Aseptic loosening rate of the humeral stem in the Coonrad-Morrey total elbow arthroplasty. Does size matter? J Shoulder Elbow Surg 2014;23:76-81. [Google Scholar]
- 23.Voloshin I, Schippert DW, Kakar S, Kaye E, Morrey B. Complications of total elbow replacement: A systematic review. J Shoulder Elbow Surg 2011;20:158-68. [Google Scholar]
- 24.Morrey BF, Adams RA, Bryan RS. Total replacement for post-traumatic arthritis of the elbow. J Bone Joint Surg Br 1991;73:607-12. [Google Scholar]
- 25.Rog D, Zuckerman LM, Riedel B. Conversion of a surgical elbow arthrodesis to total elbow arthroplasty. Case Rep Orthop 2015;2015:578189. [Google Scholar]






