
Isolated trochlear fractures are rare clinical entity, more so in an elderly lady; here is a case report of isolated trochlear fracture in a post menaupausal woman treated in a rural coal mines hospital.
Dr. Debanjan Das, Department of Orthopedics, Tata Central Hospital, Jamadoba, Jharkhand, India. E-mail: drdebanjad@yahoo.com
Introduction: Isolated trochlear fractures are very rarely reported in the orthopedic literature; moreover, most of the cases reported are of patients in the younger age group. Due to its anatomical position, trochlear fractures are usually associated with other bony injuries around the distal humerus and with elbow dislocation, and so, its extremely rare to find an isolated trochlear fracture reported in postmenopausal lady with osteoporotic bone.
Case Report:Here, we report a postmenopausal elderly lady suffering from isolated trochlear fracture of humerus trochlea. She was having pain and discomfort around her right elbow with restricted motion in elbow following a blunt trauma. After necessary investigations, we treated the patient with open reduction through posterior approach to elbow with olecranon osteotomy and fixed the fracture under direct vision with headless titanium screws. Post-operative physiotherapy was initiated after 2 weeks as pain subsided.
Conclusion: : Isolated trochlear fractures are rare clinical entity specially in postmenopausal women and it should be properly managed for a good clinical and functional outcome.
Keywords: Isolated, trochlear fracture ,elderly postmenopausal lady.
The trochlea is the medial part of distal humeral articular surface, its convex from before backwards, and concave from side to side. Its medial border is more prominent, greater in length compared to the lateral border. The grooved portion of trochlea articulates accurately with the semilunar notch of proximal ulna, its deeper and broader in the posterior aspect than the anterior, and its inclined obliquely downwards and forwards and towards the medial border of trochlea [1]. Its not having any musculoligamentous attachment and its unique presence within the olecranon fossa shield trochlea from direct trauma [2]. Again, the trochlea is shielded from sheer forces from radio capiteller joint as its forms the ulnohumeral joint [3]. Hence, trochlear fracture is usually associated with other injuries around the elbow, such as elbow dislocation, radial head fracture, and capitellum fracture. [4]. Isolated trochlear fracture is rarely reported in the literatures and how this injury actually happens is still not clear [5].
Here, we present a case report of an elderly postmenopausal lady who suffered from the right trochlear fracture, after sustaining a direct injury while being hit by a bull. She was managed surgically with headless screw fixation of the trochlea after doing the olecranon osteotomy in a rural coal mines hospital in Jharkhand, India. The purpose of this case reporting is to highlight the rarity of the reported case, the challenges in diagnosis, need for higher radiological studies, and a proper surgical plan to address the problem.
Our patient was around 55-year-old female, postmenopausal women, who was hit by a bull resulting into pain and swelling with restriction of movement of the right elbow. On examination, her right elbow was tender, and the tenderness was deep seated into the anterior aspect of the right elbow joint. The bony prominences around the elbow joint were not tender. Right elbow range of motion was 5–80° approximately in the flexion – extension plane. The pronation and supination movements were not reduced but the motion was painful. There was no open injury and the patient came to our OPD 4 days after the injury. She was hypertensive and on anti-hypertensive medication; otherwise, there was no comorbidities present.
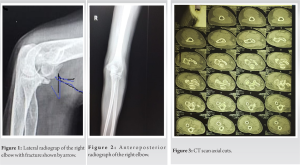
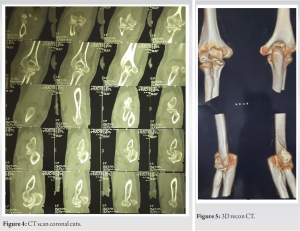
We did the anteroposterior (AP) and lateral (Lat) radiograph of the elbow. In the AP view, the fracture was hardly detectable. One has to be very careful while reading the X-ray, the Lat. View did show the fracture (Figs. 1 and 2). Hence, we did the CT scan with 3D reconstruction study which showed the true picture of the fracture (Figs. 3-5).
Surgical management
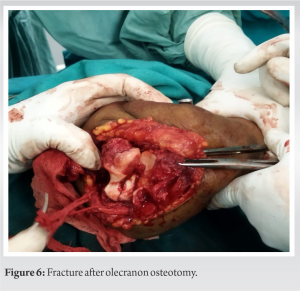
After proper counseling of the patient regarding the possibility of post-operative stiffness of the elbow and need for prolong physiotherapy, we operated the patient. She was kept in the left lateral position with arm support and general anesthesia was inducted. A posterior approach to the elbow through the olecranon osteotomy was utilized. The ulnar nerve was properly identified and isolated and protected. The fracture was identified and freshened and then temporarily fixed with K-wires (Figs. 6 and 7). Then, it was definitely fixed with 2.4 mm headless titanium screws. After that the osteotomy was fixed with 4.0 mm long cannulated cancellous screw and SS wire in figure of 8 configuration (Figs. 8 and 9). The ulnar nerve was checked for any possible compression. The elbow range of motion was checked in flexion extension plane and supination pronation plane, they were satisfactory. The wound was closed and plaster of paris posterior slab was applied with elbow at 90 flexion. The post-operative period was uneventful, wound healed nicely and stitches were off on 14th post-operative day. Elbow range of motion was started and posterior slab was discontinued.
Post-operative period
The most common problem which we encountered during the post-operative period was the elbow stiffness. The olecranon osteotomy also added to the problem. However, gradually with persisting and dedicated elbow range of motion physiotherapy our patient has able to achieve 5–100° range of motion in the flexion extension plane and full supination pronation. She had also complained of tingling and numbness in the ulnar nerve distribution that has gradually subsided with oral methylcobalamine substitution. Any sort of massage was strictly discouraged around the elbow.

Isolated trochlear fracture is very uncommonly reported in the literature. It is reported in the literature that isolated trochlear fracture may happen in both low-energy and high-energy trauma [6].
If the fall is on outstretched arm with extended elbow the longitudinal force coming through the ulna may directly be transmitted to the trochlea, with elbow in locked position, may fracture it [7]. Fracture involving both the capitellum and trochlea constitute about 1% of all elbow fracture and (3–6)% of all distal humeral fractures but isolated trochlear fracture reported incidence is very less [8-10]. Isolated fracture of humeral trochlea is a rare entity and accordingly classified as Dubberleys subtype 1T and AO-ASIF type 13.B3.2 [11, 12].
Mckee has reported six cases of distal humeral fracture where shear forces had transmitted from capitellum to trochlea resulting into trochlear fracture [7]. The trochlear fracture may also happen with fall on flexed elbow due to transmission of the force directly through the trochlear ridge. However, it is still unclear why it causes the isolated trochlear fracture, instead of involving the total trochleocapitellar block [3]. Jupiter et al. proposed the possibility that coronoid may act as a fulcrum for transmitting the force to trochlea in a flexed elbow [7].
The choice of fixation depends upon many things, but mostly the size of fragments are particularly important. Here, we used 2.4 mm headless screws. Herbert and Fisher, in 1984, demonstrated the unique design of double threaded screw which was able to sit beneath the articular surface and provide stability and compression for starting post-operative range of movements at the earliest [7]. Sen et al. have shown the usefulness of K-wires in fixation of smaller fragments which are not amenable for screw fixation [3]. Due to the paucity of literature, it is very difficult to come to a consensus regarding the best method for fixation of trochlear fractures.
Isolated trochlear fractures are very rarely reported in the literature. We need to know in detail how these fractures happen in isolation without involving the other surrounding structures. These fractures may appear subtle in the X-rays, so we need to be very careful while interpreting them. Advanced radiological studies such as CT scans and MRI may be considered to look for the minute osteoligamentous injuries. A proper diagnosis and management associated with dedicated physiotherapy should give the patient a pain free elbow having good range of motion.
Isolated trochlear fractures are rare clinical entity specially in postmenopausal women and it should be properly managed for a good clinical and functional outcome.
References
- 1.Nauth A, McKee MD, Ristevski B, Hall J, Schemitsch EH. Distal humeral fractures in adults. J Bone Joint Surg Am 2011;93:686-700. [Google Scholar]
- 2.Mehdian H, McKee MD. Fractures of capitellum and trochlea. Orthop Clin N Am 2000;31:115-27. [Google Scholar]
- 3.Sen RK, Tripahty SK, Goyal T, Aggarwal S. Coronal shear fracture of the humeral trochlea. J Orthop Surg (Hong Kong) 2013;21:82-6. [Google Scholar]
- 4.Gonçalves LB, Ring DC. Fractures of the humeral trochlea: Case presentations and review. J Shoulder Elbow Surg 2016;25:e151-5. [Google Scholar]
- 5.Zimmerman LJ, Jauregui JJ, Aarons CE. Isolated shear fracture of the humeral trochlea in an adolescent: A case report and literature review. J Pediatr Orthop B 2015;24:412-7. [Google Scholar]
- 6.Abbassi N, Abdeljaouad N, Daoudi A, Yacoubi H. Isolated fracture of the humeral trochlea: A case report and review of the literature. J Med Case Rep 2015;9:4-8. [Google Scholar]
- 7.Osman W, Braiki M, Alaya Z, Naouar N, Ben Ayeche M. Combined isolated Laugier’s fracture and distal radial fracture: Management and literature review on the mechanism of injury. Case Rep Orthop 2016;2016:7631425. [Google Scholar]
- 8.Stamatis E, Paxinos O. The treatment and functional outcome of type IV coronal shear fractures of the distal humerus: A retrospective review of five cases. J Orthop Trauma 2003;17:279-84. [Google Scholar]
- 9.Heck S, Zilleken C, Pennig D, Koslowsky TC. Reconstruction of radial capitellar fractures using fine-threaded implants (FFS). Injury 2012;43:164-8. [Google Scholar]
- 10.Faber KJ. Coronal shear fractures of the distal humerus: The capitellum and trochlea. Hand Clin 2004;20:455-64. [Google Scholar]
- 11.Dubberley JH, Faber KJ, Macdermid JC, Patterson SD, King GJ. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Jt Surg Am 2006;88:46-54. [Google Scholar]
- 12.Bandi W, Muller M. Arbeitsgemeinschaft fur osteosynthesefragen. In: Manual of Internal Fixation: Techniques Recommended by the AO Group. New York, USA: Springer; 1979. [Google Scholar]




