
Pure hyperextension injury represents an uncommon mechanism leading to long oblique metacarpal shaft fractures, highlighting the significance of recognizing, and addressing distinctive injury patterns in the diagnosis and treatment of such fractures.
Dr. Ashraf F Shaikh, Department of Orthopedics, 6th Floor New Building, Seth G.S. Medical College and King Edward VII Memorial Hospital, Acharya Donde Marg, Parel East, Mumbai, Maharashtra, India. Email: ashrafshaikh123@gmail.com
Introduction: “Joota Chori” is a traditional Indian wedding ritual which involves playful competition between the bride’s and the groom’s friends, with the aim of hiding and retrieving the groom’s shoes.
Case Report: We describe a rare case scenario wherein an orthopedic surgeon sustained a metacarpal shaft fracture while gripping the shoe and engaging in a tussle with the groom’s friends. Despite feeling a sudden snap and experiencing pain, the surgeon held onto the shoe. The subsequent diagnosis revealed a 4th metacarpal long oblique shaft fracture.
Conclusion: This case highlights the uncommon mechanism of injury involving forceful hyperextension of the MCP joint and the potential risks associated with physically intense wedding rituals. It also emphasizes the importance of adequate first aid resources and medical attention at wedding venues to promptly address musculoskeletal injuries.
Keywords: Metacarpal fracture, trauma, wedding tradition.
“Joota Chupai” or “Joota Chori” is a customary ritual in Indian weddings wherein the groom’s shoes are traditionally hidden by the bride’s sisters as he takes them off for performing the marriage rituals; the groom gets his shoes back only after he has paid a hefty sum of money for them [1, 2]. In recent times, the bride’s friends have also joined in the above activity. The groom’s friends, on the other hand, try to prevent his shoes from being stolen. This creates a playful banter between the two groups which ends up breaking the ice and eases the forming the bonds between everyone. This activity was traditionally partaken by women and, therefore, was less physically intense [3, 4]. We present a case of metacarpal shaft fracture sustained by an orthopedic surgeon (primary author of this report) due to an unusual mechanism while tussling for the groom’s shoe.
(The case is presented as a first-person account)
The destination wedding was taking place at a 5-star hotel in South Goa, India. The “Joota Chori” ritual momentum was heated up just as the groom was about to get onto the wedding mandap. As soon as the groom took his shoe off, I grasped it with both my hands. However, 4–5 of the groom’s friends immediately ambushed me, trying to snatch the shoe. My grasp on the shoe was extremely firm and I held on. In an attempt to snatch the shoe from my grip, one of them caught hold of my left 4th and 5th finger and twisted it open in extension. There was a sudden snap and both of us knew, in that moment that a bone had been broken. I still did not let go off the shoe and with some assistance from a couple of my teammates, I got free from the huddle and ran, with the prized shoe in my hand.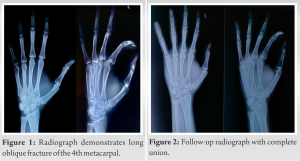
It was only then, after the adrenaline rush dropped down, that I realized the severity of pain. Being a doctor’s wedding there were about half a dozen orthopedic surgeons who witnessed the debacle, after an impromptu “clinical meet”, we decided to get an X-ray done immediately and went to the closest hospital that we could find with a decent X-ray facility by travelling 40 km to Madgaon. The journey felt longer due to the continuous discussion, where we hypothesized the character of the fracture based on the mode of trauma. The radiograph revealed (as predicted correctly) a 4th metacarpal long oblique shaft fracture (Fig. 1). Being three orthopedic surgeons, we did not bother to go back to the casualty officer. An ulnar gutter slab was applied by one of my colleagues after returning to the hotel. The 4th and 5th metacarpophalangeal joints were immobilized in 90° of flexion. The thumb, index, and middle finger were left free along with the distal interphalangeal joints of the ring and little finger. This allowed me to perform complete range of motion physiotherapy exercises throughout the duration of the immobilization and prevented any stiffness to occur. At 2 weeks, the slab was replaced with a removable ulnar gutter splint. Follow-up radiograph at 8 weeks showed complete union (Fig. 2), with a near complete functional recovery.
Metacarpal fractures account for 40% of all hand fractures. These occur most frequently due to a direct blow or crush injury (60–80%), followed by falls (10–20%) and then 5–10% of each motor vehicle accidents and sports injuries. The most common metacarpal to be fractured is the 5th, which accounts for 40% of all metacarpal fractures [5]. Typical mechanism of injury involves axial force with or without a bending component to produce a transverse fracture, usually with a dorsal apex. Spiral and oblique fractures are seen with a torsional or rotatory force given to the digit. A direct blunt force would commonly generate a comminuted or transverse fracture at the site of impact. While hyperextension injury of MCP joints is known to produce dislocations, volar capsule injury, and collateral ligament injuries, it is not a reported mechanism in the literature for metacarpal fractures [6, 7]. The fracture described in this report is a 4th metacarpal shaft long oblique fracture primarily due to forceful hyperextension of the MCP joint. Typically, this would lead to stretch on volar capsule causing its avulsion with or without MCP dislocation. In the absence of an axial impact or a significant rotational force or a direct impact on dorsum of hand, it would be counterintuitive to expect a metacarpal shaft fracture. Yet, its occurrence makes us theorize the mechanism involved here. During the act of forceful gripping of an object, the MCP joints assume an attitude of flexion due to vigorously contracted long flexor muscles. The wrist is stabilized in slight dorsiflexed attitude by simultaneous contraction of both dorsi and palmar flexors, thus synergizing the long flexor tendons for effective grip. When a hyperextension force is applied over the digit in such a state, we believe that the vigorously contracted long flexors would resist a sudden MCP hyperextension and, thus, serve to protect the volar capsule from sudden stretch and avulsion. Instead, a levering moment would be produced over the metacarpal shaft, one that effectively produces a bending force. With tightly contracted interosseous and hand intrinsic muscles, the 4th metacarpal remains sandwiched in a tight closed compartment while facing bending forces. Thus, it is unable to dissipate the forces to nearby soft tissues nor to adjacent joints (which are held rigidly stable by muscle forces). This precipitates a long oblique fracture. As a silver lining to this the contracted interosseous tissues which sandwich the metacarpal would prevent any significant displacement, we believe. This interesting course of events would probably explain a long oblique metacarpal shaft fracture with a pure hyperextension force over MCP joint. Regarding the management approach, metacarpal fractures are typically addressed non-operatively, particularly when there is minimal displacement. Immobilization techniques such as splinting or casting are commonly employed to ensure proper alignment and promote optimal healing conditions. Surgical intervention becomes a consideration in instances of displaced fractures or those involving multiple metacarpals. These can be in the form of CRIF with K-wires or plates when indicated. The origin of the “Joota Chori” tradition is not very clear, and there are various theories and stories associated with it. One theory suggests that this ritual has its roots in ancient times when marriages were often arranged between people from different villages or towns. In such cases, the groom’s family members would come to the bride’s village or town to solemnize the wedding. The bride’s family members would steal the groom’s shoes to prevent him from leaving immediately after the wedding ceremony and to encourage him to stay with the bride’s family for a while [8]. The tradition typically involves female participation, is quite playful and not highly competitive. However, over the last few years, the male members involvement has increased, which has amplified the physical intensity. This acts as a hazard for such injuries occurring during this originally light-hearted game. One might question while reading, whether this case deserves to be published in medical literature? We believe that this case has multiple important messages for Indian readers, and those dealing with athletic hand injuries. First, one must understand that the background setting in which the injury took place is noteworthy and unique to the Indian scenario. It also gives insight regarding the possibility of injury during any such competitive rituals taking place during the wedding. Second, the incident highlights the neglect and deficiency of first aid for musculoskeletal injuries at five-star hotels and popular tourist destinations in India. Grand Indian weddings often involve energetic dance performances and other activities such as which make the participants prone to injuries. Lack of basic splintage and first aid equipment at such times can prove to be costly! Similarly, the need for first aid in event of medical events such as coronary events or alcohol intoxication is invaluable. Access to such facilities is often an hour away which is a tremendous delay. Third, this case highlights how a hyperextension injury of MCP can lead to metacarpal shaft fracture, which is not reported in the literature to the best of our knowledge. This bears implication in athletic sports such as rugby where there is tussle over a ball. Finally, the fact that the primary author did not leave the fight for the shoe even after hearing and feeling the painful snap, has maybe something to do with an orthopedic surgeon’s personality trait – Full of confidence and a never dying spirit to win [9,10].
Awareness of hyperextension mechanism as an uncommon cause of metacarpal shaft fracture is worth noting. Grand Indian weddings should be equipped with relevant first aid equipment for musculoskeletal injuries. The probability of such injuries occurring in traditional Indian marriage rituals must be kept in mind, especially when there is participation of strong and spirited orthopedic surgeons.
The enthusiasm of wedding rituals, dance, and games is increasing over years, and one must keep in mind that the incidence of musculoskeletal injuries would follow the same trend. This highlights the need for adequate first aid equipment during marriages. Pure hyperextension injuries of the digits can lead to long oblique fractures of the metacarpals.
References
- 1.Patel KD. Marriage rituals and symbolism in Northern India. J South Asian Pop Cult 2011;9:23-38. [Google Scholar]
- 2.Kaur J. Wedding rituals in north India: From pre-wedding rituals to the post-wedding celebrations. Int J Multidisciplinary Res 2015;1:10-5. [Google Scholar]
- 3.Mallaiah PB. Rituals, myths and symbols in Indian weddings. Int J Humanit Soc Sci Res 2019;9:13-24. [Google Scholar]
- 4.Verma RS. Anthropological study of the ‘Joota Chupai’ ceremony in Indian weddings. Indian J Tradit Knowledge 2019;18:159-63. [Google Scholar]
- 5.Chung KC, Spilson SV. The frequency and epidemiology of hand and forearm fractures in the United States. J Hand Surg Am 2001;26:908-15. [Google Scholar]
- 6.Green DP, Hotchkiss RN, Pederson WC. Green’s Operative Hand Surgery. Ch. 7. Philadelphia, PA: Elsevier; 2017. p. 236-7. [Google Scholar]
- 7.Soong M, Got C, Katarincic J. Ring and little finger metacarpal fractures: Mechanisms, locations, and radiographic parameters. J Hand Surg Am 2010;35:1256-9. [Google Scholar]
- 8.Juneja V. Understanding Indian Weddings: Customs and Traditions. Wisdom Tree Publishers; 2015. [Google Scholar]
- 9.Klein G, Hussain N, Sprague S, Mehlman CT, Dogbey G, Bhandari M. Characteristics of highly successful orthopedic surgeons: A survey of orthopedic chairs and editors. Can J Surg 2013;56:192-8. [Google Scholar]
- 10.Phillips D, Egol KA, Maculatis MC, Roloff KS, Friedman AM, Levine B, et al. Personality factors associated with resident performance: Results from 12 accreditation council for graduate medical education accredited orthopaedic surgery programs. J Surg Educ 2018;75:122-31. [Google Scholar]






