
In the context of a patient with high-stage carcinoma and the sub-acute onset of mono or oligoarticular inflammatory arthritis, physicians should consider synovial metastases on their differential.
Andrew C Muran, MPhil Zucker School of Medicine at Hofstra-Northwell Health, 500 Hofstra University, Hempstead, NY, 11549, USA. E-mail: amuran@northwell.edu
Introduction: This case report describes the third documented example of primary esophageal carcinoma metastasizing to the patella and the first documented example of esophageal carcinoma metastasizing to synovium.
Case Report: A 67-year-old man with a history of metastatic esophageal carcinoma presents with right knee pain and an aggressive, destructive lesion involving the superior patella. Biopsy revealed esophageal carcinoma. After ineffective radiation, he underwent resection of the tumor-filled bone and quadricep advancement. Two months later, a recurrent tumor involving the entire patella and significant knee synovitis was observed. He underwent a total patellectomy with a radical anterior synovectomy. Further assessment showed that the entire synovium was replaced with metastatic carcinoma.
Conclusion: This report describes an atypical presentation of metastasis with patella and synovium involvement.
Keywords: Esophageal carcinoma, patellar metastases, synovial metastases.
Primary patellar tumors are rare, and patellar metastases are even rarer [1, 2]. A recent literature review reported only 44 cases of patellar metastasis in the literature [2]: They found that patellar metastasis was most commonly of lung origin (~40%) and only rarely from gastrointestinal primary cancers –with esophageal carcinoma comprising <5% of patellar metastases. Although patellar metastasis is rare, even more rare is metastasis to the knee joint synovium. There appear only approximately 50 reported cases of metastasis to synovium [3] with primary lung cancer the most common cause of synovial metastasis, followed by cancers of colorectal origins, and no reported cases of upper gastrointestinal tumors metastasizing to the synovium. The purpose of this case report is to describe the third documented example of primary esophageal carcinoma metastasizing to the patella and the first documented example of esophageal carcinoma metastasizing to synovium.
The patient, who provided consent for this report, is a 67-year-old male with a past medical history of hypertension, hypothyroidism, and esophageal carcinoma with known lung metastases who presented with 3 months of worsening right knee pain. In addition, he reported that the pain worsened with any range of motion activities, as well as direct pressure, and he was unable to find any relieving factors. On examination, the patient was generally deconditioned and able to stand with significant pain. He had decreased active (10–70°) and passive range of motion (0–90°) and was otherwise neurovascularly intact without lymphadenopathy. An magnetic resonance imaging (MRI) before presentation demonstrated a 4.2 cm destructive lesion at the superior pole of the patella, invading inferiorly into the patella, along with soft-tissue involvement of the quadriceps tendon (Fig. 1). Radiographs at presentation demonstrated a radiolucent bone lesion at the superior pole of the patella (Fig. 2). Due to the rarity of patellar metastases, the patient was scheduled for a biopsy with a frozen section with a plan for exploration, curettage with bone grafting and quad augmentation if the lesion was found to be metastatic carcinoma.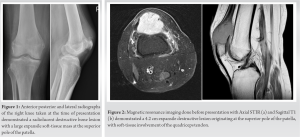
Due to medical issues, 6 weeks later the patient underwent the procedure described above. A 2-cm incision was made over the patella using fluoroscopic guidance. On dissecting through the retinaculum, abnormal tissue was noted at the superior patella. This tissue was biopsied and histologic analyses of the frozen section confirmed metastatic carcinoma. The rest of the patella was then exposed by dissecting through the retinaculum and intralesional curettage was performed. Approximately 40% of the patella was left intact. Deep into the synovial tissue, there was intact cartilage connected to the distal pole of the patella, which was left intact. Hydrogen peroxide was used to clean the wound and the joint was visualized with no significant abnormalities noted. The quadriceps tendon was then debrided and advanced to the superior pole of the patella using No. 5 Fiberwire (Arthrex, Naples, FL) in a Krackow fashion and secured distally through transosseous drill holes. The patient’s wound was closed, and he was transferred to the PACU in stable condition.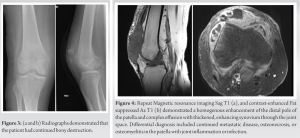
Two weeks later, the patient returned to the office for a routine follow-up. He was in considerable pain but otherwise was doing well. The wound was clean, dry, and intact. Official pathology results were reviewed with the patient confirming metastatic squamous cell carcinoma to the bone. Within the next month, the patient was admitted to an outside hospital for COVID-19 pneumonia. During the admission, there was a concern for septic arthritis as there was a poke-hole sinus tract on the anterior knee. However, arthrocentesis produced a negative cell count and culture. He also had a computed tomography which was read as concerning for osteomyelitis versus worsening malignancy. On transfer to our institution, radiographs (Fig. 3a and b) demonstrated that the patient had continued bony destruction. Repeat MRI (Fig. 4a and b) demonstrated homogenous enhancement of the distal pole of the patella with a differential diagnosis of continued metastatic disease, osteonecrosis, or osteomyelitis in the patella. The knee joint showed a large diffuse hypertrophic synovitis. Due to persistent pain, the patient was offered knee exploration and palliative completion patellectomy.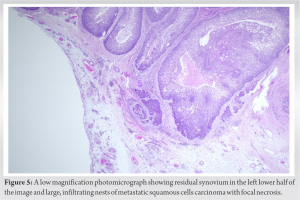
The patient had his sinus tract excised. Dissection revealed a small proximal remainder of the patella attached to the quadriceps tendon in the area of the previous advancement with significant distal bone loss. All remaining patella was removed as it had been completely replaced with a tumor. On removing the bone, the synovium was noted to have an abnormal red, beefy, nodular appearance. An extensive synovectomy was performed, including extensive superior proliferation in the suprapatellar pouch as well as the medial and lateral gutters and intercondylar notch. No purulence was encountered. Hydrogen peroxide was used to gain control of the tumor. A V-Y quadricepsplasty was performed to advance the quad tendon to the patellar tendon and close the joint. The patella and synovium were sent for pathology. The patient was kept in extension and allowed to weight bear. His pain was better controlled although his ambulation was limited. He expired 3 months post-operation due to pulmonary complications.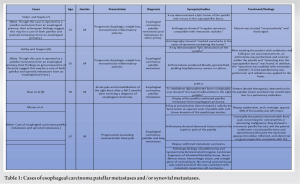
Final pathology showed irregular, tan-brown fragments of lobulated fibrofatty tissue, dense fibrous tissue, hemorrhagic tissue, and a single piece of 3.9 × 3.2 × 2.0 cm of cortical bone, all replaced with tumor (Fig. 5). No normal synovial tissue was noted, with all abnormal periarticular soft-tissue consistent with disseminated metastatic squamous cell carcinoma.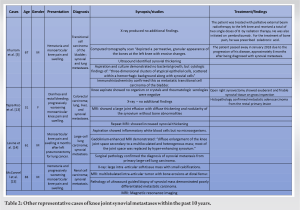
To the best of our knowledge, this case report is the fourth well-documented case of patellar metastasis and the first well-documented case of synovial carcinomatosis. Metastasis with esophageal carcinoma is common with up to 50% of diagnosed patients having metastasis to other organs [4]. Lung metastasis as seen in this case is fairly common, occurring in 6.5% of patients diagnosed with esophageal carcinoma [5]. Although bone is the second-most common place for metastasis of esophageal carcinoma, rarely does this occur in the patella or knee synovium [4]. Patella tumors in general are rare entities and are rarely metastatic in origin. Prior reviews from 1900 to 2000 reported 384 cases, and only 12% of these tumors were metastatic in origin [6]. An epidemiological study showed that patellar metastasis is most commonly of lung (~35%), breast (~10%), or kidney (~10%) origin [6]. Esophageal carcinoma reportedly occurs at an incidence of 7%, with only three other cases found in the literature (Table 1) [7, 8, 9]. Consistent with prior reports, our patient presented with disabling knee pain, a radiolucent lesion in the patella, and MRI-revealed non-specific hypertrophic synovitis. Despite aggressive initial surgical treatment, the patient developed tumor progression to the inferior pole of the patella, requiring intervention for persistent pain. During subsequent patellectomy with V-Y advancement, the synovial tissue was noted as grossly abnormal and friable, and a full synovectomy was performed. Pathologic analysis confirmed the presence of synovial metastasis with a special note of no remaining normal synovial tissue. Metastasis of solid tumors to synovium is similarly a rare event with approximately 50 cases described in the literature (Table 2) [3, 10]. These are most commonly of lung or colorectal origin [3]. To the best of our knowledge, this is the first case report on esophageal carcinoma metastasizing to synovium. Prior studies have suggested two mechanisms by which tumors metastasize to synovial tissue including direct spread from periarticular masses (likely what happened in our case) versus hematogenous spread [11, 12], while others have suggested prior surgical intervention played a role in spread to synovium [6]. Although the etiology and timeline of synovial metastasis, in this case, is unknown, the pathologist was unable to identify any normal synovial tissue in the specimen, suggesting the synovial metastasis was either present for a long period of time or was rapidly aggressive, representing a case of synovial carcinomatosis. The initial and follow-up MRI scans showed enhancement throughout the synovium, which could be consistent with both synovitis versus disseminated synovial metastases (Figs. 1, 4a and b). Physicians treating such patients should consider co-incidence of synovial metastasis and be sensitive to synovial biopsy or prophylactic synovectomy in patients undergoing surgical intervention. Furthermore, as disseminated carcinoma in other body cavities has been well described (for example, pleural or peritoneal carcinomatosis), we suggest a new diagnosis of “synovial carcinomatosis.”
Patellar and synovial metastases are rare events, and their co-incidence is even rarer. As a result, the approach to diagnosing and treating either metastatic event remains understudied. This highlights the importance of publishing detailed reports on the treatment of patients with these conditions. Here, we have presented such a case, possibly the third to be published, and the first to be diagnosed definitively as concurrent patellar and synovial metastases, with the synovium completely replaced with carcinoma. Both metastases appear to present similarly, albeit non-specifically, with the sub-acute onset of mono or oligoarticular inflammatory arthritis. However, in the context of a previous diagnosis of high-stage carcinoma, physicians should consider either patellar or synovial metastases in their differential.
Synovial metastases are rare occurrences, but in the context of a patient with previously diagnosed high-stage carcinoma, and sub-acute to chronic inflammatory arthritis, they should be considered. Our case is one of a few well-documented descriptions of the diagnostic workup and management of a patient with synovial and patellar metastases from esophageal carcinoma – offering insight into how these patients might present, the diagnostic tests that can be used, pathologic descriptions of these lesions, and discussion of their surgical management. Though definitive diagnosis of synovial metastases requires a biopsy of the tissue, soft-tissue involvement can be visualized with MRI and help to narrow the differential to a process involving periarticular soft tissue. Lastly, due to the rarity of synovial and patellar metastases in the literature, and the significant diagnostic and treatment challenges they pose, it is important for physicians who encounter patients with these conditions to publish detailed case reports on how they were diagnosed and treated.
References
- 1.Choi M, Probyn L, Rowbottom L, McDonald R, Bobrowski A, Chan S, et al. Clinical presentations of below knee bone metastases: A case series. Ann Palliat Med 2017;6:S85-9. [Google Scholar]
- 2.Li G, Shan C, Sun R, Liu S, Chen S, Song M, et al. Patellar metastasis from primary tumor. Oncol Lett 2018;15:1389-96. [Google Scholar]
- 3.Khurram R, Khurram A, Chaudhary K. Index case of synovial metastasis in a patient with transitional cell carcinoma of the bladder. BMJ Case Rep 2020;13:e235084. [Google Scholar]
- 4.Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med 2003;349:2241-52. [Google Scholar]
- 5.Guo J, Zhang S, Li H, Hassan MO, Lu T, Zhao J, et al. Lung metastases in newly diagnosed esophageal cancer: A population-based study. Front Oncol 2021;11:603953. [Google Scholar]
- 6.Mercuri M, Casadei R. Patellar tumors. Clin Orthop Relat Res 2001;389:35-46. [Google Scholar]
- 7.Stoler B, Staple TW. Metastases to the patella. Radiology 1969;93:853-6. [Google Scholar]
- 8.Ashby ME, Dappen N. Esophageal carcinoma metastatic to the patella. A case report. JAMA 1976;235:2519-20. [Google Scholar]
- 9.Zhao Y, Zhang Q, Feng H, Zhu X. Oesophageal carcinoma with solitary patellar metastasis: A rare case report. J Int Med Res 2021;49:3000605211009812. [Google Scholar]
- 10.Currall VA, Dixon JH. Synovial metastasis: An unusual cause of pain after total knee arthroplasty. J Arthroplasty 2008;23:631-6. [Google Scholar]
- 11.Younes M, Hayem G, Brissaud P, Grossin M, Kahn MF, Meyer O. Monoarthritis secondary to joint metastasis. Two case reports and literature review. Joint Bone Spine 2002;69:495-8. [Google Scholar]
- 12.Evans PD, Mintowt-Czyz WJ. Late metastasis of carcinoma of the colon to the knee. J R Coll Surg Edinb 1987;32:123-4. [Google Scholar]
- 13.Tapia Rico G, Klevansky M, Townsend A, Price T. Synovial metastasis of the knee in a KRAS mutant rectal adenocarcinoma patient. BMJ Case Rep 2017;2017:bcr2017220008. [Google Scholar]
- 14.Levine HR, Tingle E, Carter B, Dockery D. Synovial metastasis from lung cancer. Proc (Bayl Univ Med Cent) 2013;26:25-7. [Google Scholar]
- 15.McConnell M, Kumar R, Amini B, Lin PP, Wang WL. Calcified synovial metastasis in the knee from renal cell carcinoma: A case report. Skeletal Radiol 2017;46:123-7. [Google Scholar]





