
The establishment of a criterion for muscle compartment pressure checks is crucial in avoiding any neuromuscular damage in patients who present with rare cases of acute exertional compartment syndrome.
Dr. Kanwar Partap S Parhar, Washington State University, Elson S. Floyd College of Medicine, Spokane, Washington, USA. E-mail: kanwarpartap.parhar@wsu.edu
Introduction: Acute exertional compartment syndrome (AECS) is a condition with the potential for devastating outcomes if not promptly treated. Physicians must maintain a high index of suspicion when evaluating patients presenting with pain, swelling, decreased range of motion, and numbness within a muscle compartment. However, AECS is frequently misdiagnosed due to a multitude of factors, leading to a delay in treatment. In this case report, we would like to shed light on a rare case of bilateral upper-extremity AECS and suggest the treatment paradigm we believe will help prevent negative outcomes.
Case Presentation: A previously healthy 33-year-old male presented with bilateral weakness, tingling, tenderness, swelling, and pain upon movement in the trapezius and deltoid muscles. The symptoms started after he performed “burpees” for 18 h following a 12-h forest-fire firefighting shift. The patient’s rapidly developing clinical presentation warranted compartmental pressure checks for suspicion of AECS. Being able to quickly determine the elevated trapezius, deltoid, and supraspinatus compartmental pressures allowed us to perform immediate bilateral fasciotomies with delayed primary closure to relieve compartment pressure.
Conclusion: The delay in treatment for patients presenting with AECS is multifactorial and may lead to devastating outcomes if not promptly addressed. The lack of literature regarding bilateral upper-extremity AECS makes the treatment for this condition even more difficult. For our patient, having a proper criterion for performing compartmental pressure checks played a vital role in ensuring an accurate diagnosis and timely medical intervention.
Keywords:Compartment syndrome, acute compartment syndrome, acute exertional compartment syndrome, fasciotomy.
Acute compartment syndrome (ACS) is a pathological condition characterized by heightened pressure within a closed osteofascial compartment, leading to compromised local circulation. The increased pressure impedes normal blood flow, leading to pain, swelling, decreased ROM, numbness, and paresthesia in the affected muscles. If not promptly treated, this can result in tissue ischemia and, ultimately, irreversible tissue necrosis [1]. ACS is a condition that is most often seen in young males, with an annual incidence of 7.3 people per 100,000 males [2]. ACS can occur due to trauma, acute traumatic compartment syndrome (ATCS), or due to over-exertion, acute exertional compartment syndrome (AECS). Both forms are damaging and can lead to severe neuromuscular injuries. But unlike ATCS, which is related to a traumatic incident and often has a clear diagnosis, AECS is a diagnosis of exclusion, which requires physicians to maintain a high index of suspicion when evaluating patients. Unfortunately, AECS is often misdiagnosed, leading to many cases of irreparable harm that could have been prevented [3]. The reasons for these misdiagnoses are many. First, there is a lack of awareness among providers, with limited reported cases and available literature on appropriate diagnosis and management criteria. Second, in terms of causes of ACS, AECS has a significantly smaller prevalence when compared to ATCS. Traumatic fractures causing ATCS compromise around 75% of the ACS cases, with tibial shaft fractures being the most common cause [4, 5, 6]. Third, the presentation of AECS is most often seen in the lower extremities in the setting of exercise-related leg pain, making the occurrence and reporting of upper extremity cases very rare [7]. Finally, the presentation of a patient with compartment syndrome (CS) due to exertion is most often seen in cases of chronic exertion, chronic exertional CS (CECS). Compared to CECS, AECS is seen far less, and its treatment has been shown to be delayed in many cases as well [8]. When a diagnosis of AECS is made, it is initially managed conservatively. When conservative treatment fails, a fasciotomy is performed to relieve compartmental pressure. While the fasciotomy for CECS is an elective procedure, patients with AECS require an emergent fasciotomy due to the severity of the outcomes. The time sensitivity due to ongoing ischemia, paired with the mentioned misdiagnosis reasons, is what leads to unfavorable outcomes in many patients [9]. This begs the need for a review of the current treatment protocol. In this case report, we shed light on the importance of clinicians maintaining a strong clinical suspicion of AECS and our recommendation on compartmental pressure check criteria in a rare case of bilateral upper-extremity AECS.
A previously healthy 33-year-old male presented to the emergency department with bilateral weakness, tingling, tenderness, swelling, and pain with movement of the trapezius and deltoid muscles, along with slight numbness in his hands. The patient reported the sudden onset of his symptoms after performing “burpees” for 18-h straight directly after a 12-h forest-fire firefighting shift.” The physical examination was positive for decreased range of motion, swelling, numbness, weakness, bilateral cyanosis, and pain in the shoulders bilaterally, right greater left; pain was rated at 7/10 in severity. On admission, laboratory studies showed elevated SGPT/ALT of 77 units/L and SGOT/AST of 253 units/L (GFR est: 103, K+: 4.0, Ca2+: 9.3, albumin: 4.3) and elevated CK results. Specifically, the CK was 28,598 units/L on the first blood draw and 26,787 units/L on the second blood draw 2-h later. The patient’s CBC, urinalysis, and ECG were unremarkable. Radiographic imaging included magnetic resonance imaging (MRI) without contrast to determine the extent of muscle damage. MRI of the left shoulder showed an increased T2 signal and overall size of the supraspinatus portion of the rotator cuff, with some involvement of the anterior third of the deltoid muscle (Fig. 1).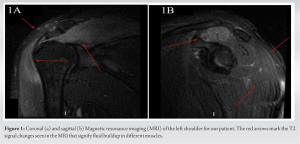 Abnormal thickening and severe tendinitis were also seen in the subscapularis, supraspinatus, and infraspinatus portions of the rotator cuff. Similarly, the right shoulder MRI showed an increased T2 signal and overall size of the supraspinatus portion of the rotator cuff, the superior portion of the infraspinatus, and portions of the anterior and middle deltoid muscles. The rotator cuff also showed significant tendinitis involving the supraspinatus and infraspinatus, with lesser involvement of the subscapularis (Fig. 2).
Abnormal thickening and severe tendinitis were also seen in the subscapularis, supraspinatus, and infraspinatus portions of the rotator cuff. Similarly, the right shoulder MRI showed an increased T2 signal and overall size of the supraspinatus portion of the rotator cuff, the superior portion of the infraspinatus, and portions of the anterior and middle deltoid muscles. The rotator cuff also showed significant tendinitis involving the supraspinatus and infraspinatus, with lesser involvement of the subscapularis (Fig. 2). 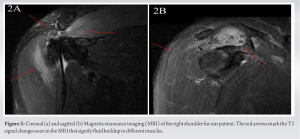 The patient’s history, laboratory, and radiographic findings made us suspect AECS to be the causative factor for which compartmental pressure checks were done. The Stryker compartment measuring system showed the right trapezius, deltoid, and supraspinatus pressures to be approximately 55–60 mmHg. In the left shoulder, the trapezius, deltoid, and supraspinatus showed pressures between 20 and 25 mmHg. Elevated compartment pressures suggested the need for a decompressive fasciotomy with delayed primary closure. This procedure was performed on the right shoulder the 1st day and on the left shoulder the following day due to the progression of symptoms. After appropriate draping and preparation, an incision was made just anterior and superior to the spine of the scapula, and the trapezius muscle was elevated from the anterosuperior aspect of the scapular spine to achieve decompression of the supraspinatus. The deltoid fascia was incised longitudinally in areas displaying increased uptake on the MRI. The fasciotomy wounds were closed approximately 1 week later on both sides. Electrical stimulation showed activity in both the trapezius, deltoid, and parts of the supraspinatus. After surgery, the patient was advised to avoid any intense physical activity and to follow-up with physical therapy. The 1-month post-operative evaluation showed great ROM and strength in both his shoulders, each with an American Shoulder and Elbow Surgeons (ASES) score of 68. The scores range from 0 to 100; a higher score indicates a better shoulder condition [10]. The patient’s 6-month evaluation showed no pain, swelling, redness, or warmth in his shoulders bilaterally, with ASES scores of 73. Although the patient did complain of having numbness and tingling around his anterior neck and chest and had a positive carpal tunnel compression test. A nerve conduction test for both upper extremities was ordered to further investigate this; however, for unspecified reasons, the patient did not follow-up with this appointment. Nevertheless, we suspect the above issues to be due to a residual injury to his brachial plexus secondary to the AECS. The vagueness of the symptoms deterred us from considering surgery to be the cause of these symptoms. On a final follow-up 4 years after the surgery, the patient had recovered well and was well beyond being medically stationary. He still complained about a variety of severe neuromusculoskeletal issues. These issues were unrelated to his diagnosis, and despite being objectively healed, we suspect some worker’s compensation psychology is at play here, as it was covered by the Department of Labor and Industry [11]. The whole-person impairment rating was used to determine the extent of permanent damage in the patient. The percentage calculated reflects how much their body was affected. During this visit, a rating of 12% was calculated, and it was concluded that no further treatment could be done to further the patient’s recovery [12].
The patient’s history, laboratory, and radiographic findings made us suspect AECS to be the causative factor for which compartmental pressure checks were done. The Stryker compartment measuring system showed the right trapezius, deltoid, and supraspinatus pressures to be approximately 55–60 mmHg. In the left shoulder, the trapezius, deltoid, and supraspinatus showed pressures between 20 and 25 mmHg. Elevated compartment pressures suggested the need for a decompressive fasciotomy with delayed primary closure. This procedure was performed on the right shoulder the 1st day and on the left shoulder the following day due to the progression of symptoms. After appropriate draping and preparation, an incision was made just anterior and superior to the spine of the scapula, and the trapezius muscle was elevated from the anterosuperior aspect of the scapular spine to achieve decompression of the supraspinatus. The deltoid fascia was incised longitudinally in areas displaying increased uptake on the MRI. The fasciotomy wounds were closed approximately 1 week later on both sides. Electrical stimulation showed activity in both the trapezius, deltoid, and parts of the supraspinatus. After surgery, the patient was advised to avoid any intense physical activity and to follow-up with physical therapy. The 1-month post-operative evaluation showed great ROM and strength in both his shoulders, each with an American Shoulder and Elbow Surgeons (ASES) score of 68. The scores range from 0 to 100; a higher score indicates a better shoulder condition [10]. The patient’s 6-month evaluation showed no pain, swelling, redness, or warmth in his shoulders bilaterally, with ASES scores of 73. Although the patient did complain of having numbness and tingling around his anterior neck and chest and had a positive carpal tunnel compression test. A nerve conduction test for both upper extremities was ordered to further investigate this; however, for unspecified reasons, the patient did not follow-up with this appointment. Nevertheless, we suspect the above issues to be due to a residual injury to his brachial plexus secondary to the AECS. The vagueness of the symptoms deterred us from considering surgery to be the cause of these symptoms. On a final follow-up 4 years after the surgery, the patient had recovered well and was well beyond being medically stationary. He still complained about a variety of severe neuromusculoskeletal issues. These issues were unrelated to his diagnosis, and despite being objectively healed, we suspect some worker’s compensation psychology is at play here, as it was covered by the Department of Labor and Industry [11]. The whole-person impairment rating was used to determine the extent of permanent damage in the patient. The percentage calculated reflects how much their body was affected. During this visit, a rating of 12% was calculated, and it was concluded that no further treatment could be done to further the patient’s recovery [12].
Our patient’s case demonstrated a rare situation of bilateral upper-extremity AECS that required immediate fasciotomies. Although AECS in the legs is quite common, AECS of the deltoid is far rarer, with only 20 previous cases reported [13]. Despite CS being a fundamental concept in orthopedics, the progress or change in the treatment paradigm has been the same since the 1970s. This lack of progression and proper management of CS and its subtypes has led to many cases of delayed treatment with negative outcomes. In a report by Liu et al., a patient with an initial misdiagnosis of a muscle strain delayed AECS treatment by 8 days. The delay led to severe neuromuscular injuries, requiring a necrotic muscle debridement procedure and a 3-month recovery time to recuperate from the deficits [14]. Through our patient’s case, we would like to go over some of the important findings and considerations we made in the course of their treatment. The evaluation of AECS starts with a thorough history and physical examination, with symptoms of AECS presenting as early as a few hours to up to 48-h after the incident [2]. The history of an intense firefighting shift followed by “burpees” for 18-h straight created the initial consideration for AECS in our differentials. Its manifestation has been remembered by “The five P’s”, (pain, pulselessness, paresthesia, paralysis, and pallor) over the affected muscle compartments [15]. Our patient presented with four of the five P’s, with pulses intact in both of the upper extremities. Along with the physical exam, laboratory tests and radiological findings can aid in the diagnosis of AECS, both of which were abnormal in our patient. However, these tests have limited sensitivity and specificity to confirm a diagnosis of AECS. A definitive diagnosis can be made by measuring the intercompartmental pressures of the suspected muscles. The modified Pedowitz criteria are the most widely used criteria to obtain and rule out a diagnosis of AECS in the compartment of interest. A diagnosis of AECS is made if pressures are >15 mmHg at rest, >30 mmHg after 1 min of exercise, or >20 mmHg after 5 min of exercise [16-18]. However, this criterion lacks guidelines on whom to perform compartment pressure checks and provides no insight on performing compartmental pressure checks that may not require a fasciotomy. Our suggestion for the change in treatment paradigm is from the work of Matsen et al., in which they start by providing clear initial indicators for performing a compartmental pressure check. These are: (1) the evaluation of a compartment in which the diagnosis of CS cannot be made or ruled out with clinical certainty; (2) The prospective evaluation of a compartment at high risk, as in a patient with a severely swollen limb but with no neural deficits [19]. Once a patient meets the criteria and compartmental pressure checks are performed, they consider the threshold for CS with an emergent fasciotomy to be 45 mmHg. In one study, they used the above indications to identify 31 patients, of whom 14 presented with clinical findings of CS and had compartment pressures exceeding 45 mmHg. The remaining 17 presented with abnormal compartment pressures exceeding 20 mmHg and did not have CS but were at high risk for it. Doing so allowed them to perform immediate fasciotomies on the 14 patients, drastically minimizing the risk of any neuromuscular injuries. Moreover, the reading of abnormal compartmental pressures in the remaining 17 patients allowed them to remain vigilant if the symptoms were to progress. From this, it is implicit that the performance of pressure checks in compartments that do not require a fasciotomy is appropriate. Following the indications above, compartmental pressure checks were performed and found to be between 55 and 60 mmHg in the right trapezius, deltoid, and supraspinatus at rest. In the left shoulder, the trapezius, deltoid, and supraspinatus all showed pressures between 25 and 20 mmHg. This finding allowed us to confirm our diagnosis of the right shoulder and proceed to perform an emergent fasciotomy for decompression. Importantly, the following day, the left shoulder showed progression in symptoms and presented similarly to the right shoulder. This progression, along with the previous diagnosis of AECS in the right shoulder, allowed us to make the same diagnosis, and a fasciotomy to decompress the muscle compartments was performed immediately. In our experience, the confirmation of AECS through compartmental pressure checks played a crucial role in the initiation of early treatment, as the time between the onset of symptoms and performing a fasciotomy has been shown to be a strong predictor of outcomes in patients with AECS [19]. By maintaining a high index of suspicion for AECS and following the treatment paradigm above, we believe this allowed us to provide our patient with the appropriate care promptly, reducing the time to surgery and helping prevent any serious outcomes.
The presentation and management of AECS bilaterally in the upper extremities are very limited in the current literature, making the management of such a devastating condition difficult. Early diagnosis and treatment are crucial to prevent any long-term neuromuscular damage in such cases. We believe that the indications we followed for compartmental pressure checks and performing a fasciotomy allowed us to do so, giving our patient a positive outcome.
Managing bilateral upper-extremity AECS can be difficult due to the lack of literature and complex presentation. We believe the two primary indications for checking compartmental pressures are: (1) when the diagnosis of CS cannot be conclusively made based on clinical assessment. (2) When evaluating compartments at high risk, present several physical exam symptoms. Following this criteria for compartmental pressure checks for patients with AECS allowed us to avoid long-term damage to our patients’ health.
References
- 1.Varacallo M, Shirey L, Kavuri V, Harding S. Acute compartment syndrome of the hand secondary to propofol extravasation. J Clin Anesth 2018;47:1-2. [Google Scholar]
- 2.Torlincasi AM, Lopez RA, Waseem M. Acute compartment syndrome. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448124 [Last accessed on 2023 Jan 16]. [Google Scholar]
- 3.Lundy DW, Bruggers JL. Management of missed compartment syndrome. In: Mauffrey C, Hak DJ, Martin MP 3rd, editors. Compartment Syndrome: A Guide to Diagnosis and Management. Cham, CH: Springer; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553895 [Last accessed on 2023 Jan 16]. [Google Scholar]
- 4.Park S, Ahn J, Gee AO, Kuntz AF, Esterhai JL. Compartment syndrome in tibial fractures. J Orthop Trauma 2009;23:514-8. [Google Scholar]
- 5.Patel RV, Haddad FS. Compartment syndromes. Br J Hosp Med (Lond) 2005;66:583-6. [Google Scholar]
- 6.Oliver JD. Acute traumatic compartment syndrome of the forearm: Literature review and unfavorable outcomes risk analysis of fasciotomy treatment. Plast Surg Nurs 2019;39:10-3. [Google Scholar]
- 7.Diebal AR, Gregory R, Alitz C, Gerber JP. Forefoot running improves pain and disability associated with chronic exertional compartment syndrome. Am J Sports Med 2012;40:1060-7. [Google Scholar]
- 8.Hope MJ, McQueen MM. Acute compartment syndrome in the absence of fracture. J Orthop Trauma 2004;18:220-4. [Google Scholar]
- 9.Livingston KS, Meehan WP 3rd, Hresko MT, Matheney TH, Shore BJ. Acute exertional compartment syndrome in young athletes: A descriptive case series and review of the literature. Pediatr Emerg Care 2018;34:76-80. [Google Scholar]
- 10.Michener LA, McClure PW, Sennett BJ. American shoulder and elbow surgeons standardized shoulder assessment form, patient self-report section: Reliability, validity, and responsiveness. J Shoulder Elbow Surg 2002;11:587-94. [Google Scholar]
- 11.Fujihara Y, Shauver MJ, Lark ME, Zhong L, Chung KC. The effect of workers’ compensation on outcome measurement methods after upper extremity surgery: A systematic review and meta-analysis. Plast Reconstr Surg 2017;139:923-33. [Google Scholar]
- 12.Cocchiarella L, Lord SJ. 16-3. In Guides to the Evaluation of Permanent Impairment. 5th ed. Philadelphia, PA: AMA Press; 2002. [Google Scholar]
- 13.Kooner S, Crocker D, Matthewson G, Byers B, Desy NM. Ipsilateral deltoid and hand compartment syndrome: A case report and review of the literature. JBJS Case Connect 2020;10:e0289. [Google Scholar]
- 14.Liu S, Wang C, Song W, Wang J, Zhao S. A case report of delayed treatment of acute exertional osteofascial compartment syndrome in the anterior compartment of the calf. Medicine (Baltimore) 2022;101:e32449. [Google Scholar]
- 15.Guo J, Yin Y, Jin L, Zhang R, Hou Z, Zhang Y. Acute compartment syndrome: Cause, diagnosis, and new viewpoint. Medicine (Baltimore) 2019;98:e16260. [Google Scholar]
- 16.Broadhurst PK, Robinson LR. Compartment syndrome: Neuromuscular complications and electrodiagnosis. Muscle Nerve 2020;62:300-8. [Google Scholar]
- 17.Chatterjee R. Diagnosis of chronic exertional compartment syndrome in primary care. Br J Gen Pract 2015;65:e560-2. [Google Scholar]
- 18.Pedowitz RA, Hargens AR, Mubarak SJ, Gershuni DH. Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med 1990;18:35-40. [Google Scholar]
- 19.Matsen FA, Winquist RA, Krugmire RB. Diagnosis and management of compartmental syndromes. J Bone Joint Surg Am 1980;62:286-91. [Google Scholar]







