
Chronic DRUJ injuries can be treated well using tight-rope technique with better outcome and early rehabilitation.
Dr. Nishant Jaiswal, Department of Orthopaedics, Government Medical College, Nagpur, Maharashtra, India. E-mail: nishant.jaiswa36@gmail.com
Introduction: The Galeazzi fracture is a fracture of the middle to distal one-third of the radius associated with dislocation or subluxation of the distal radioulnar joint (DRUJ) associated with high energy trauma. Injury to the dynamic and static stabilizers of DRUJ if unnoticed or poorly treated may lead to chronic instability which in turn can cause chronic pain and disability due to stiffness, decreased grip strength, forearm rotation, and symptomatic osteoarthritis
Case Report: A 35-year-old gentleman sustained trauma after fall from a motorcycle presented after 2 months with radiology suggestive of midshaft radius fracture with dorsal DRUJ dislocation treated with open reduction, internal fixation with DRUJ reconstruction using a novel technique not described before in any literature. After 3 months, the patient had significant pain relief at the wrist joint and regained painless, near normal range of motion at the wrist joint with good hand grip. The patient showed improvement in radiological and functional scores.
Conclusion: Reconstruction of DRUJ using this novel technique provides good functional outcome including pain relief, improvement in hand grip and movements at the wrist and elbow joint similar to conventional techniques of intra as well as extra-articular tenodesis without causing donor site morbidity to the patient with lesser instrumentations and significantly reduced operating time.
Keywords: Galeazzi fracture–dislocation, DRUJ instability, DRUJ reconstruction.
The Galeazzi fracture is a fracture of the middle to distal one-third of the radius associated with dislocation or subluxation of the distal radioulnar joint (DRUJ) associated with high-energy trauma [1]. Galeazzi fractures account for approximately 7% of all forearm fractures in adults. Distal radius fractures are far more common than midshaft radius fractures [2]. Findings suggestive of DRUJ injury on plain radiographs include radius shortening >5 mm relative to the ulna, fracture of the base of the ulnar styloid, asymmetry compared to the contralateral uninjured limb radiographs, widening of the DRUJ on anteroposterior radiographs, and lateral radiographs subluxation or dislocation of the radius relative to the ulna [3]. Injury to the dynamic and static stabilizers of DRUJ if unnoticed or poorly treated may lead to chronic instability which in turn can cause chronic pain and disability due to stiffness, decreased grip strength with forearm rotation, and symptomatic osteoarthritis [4].
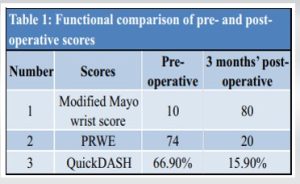
We hereby present a case of 35-year-old gentleman, a four-wheeler driver by occupation who sustained trauma to his right forearm after an alleged history of fall from his motorbike diagnosed as right-sided comminuted midshaft radius fracture and associated dorsal DRUJ dislocation (Galeazzi fracture dislocation). He was advised surgery for the same at a local hospital but he denied any surgical treatment and opted to be treated by a local osteopath. The patient presented to our outpatient department 2 months later with complaints of painful movements at the wrist and forearm fixed in mid-prone position with mild angular deformity appreciated in the forearm. Radiologically, malunion of the radial shaft with dorsal dislocation of DRUJ was evident (Fig. 1). On assessment “Modified Mayo-wrist score” was 10 (Poor), patient-rated wrist evaluation score (PRWE) was 74 (higher the score, worse is the outcome) and Quick-DASH score was 66.9% (lower the score, better the outcome). The patient was offered surgical intervention in the form of open reduction internal fixation with DRUJ reconstruction if required.
On assessment “Modified Mayo-wrist score” was 10 (Poor), patient-rated wrist evaluation score (PRWE) was 74 (higher the score, worse is the outcome) and Quick-DASH score was 66.9% (lower the score, better the outcome). The patient was offered surgical intervention in the form of open reduction internal fixation with DRUJ reconstruction if required.
Through Modified Henry’s approach, the fracture site was exposed and found to be malunited. The fracture site was osteotomized using osteotome, reduced, and fixed using a 7-hole 3.5 mm DCP plate with local site bone grafting done. Restoration of radial bow and radial height was confirmed under a fluoroscope (Fig. 2). The wound was closed in layers. Next, the stability of DRUJ was assessed with the wrist in the prone position. The piano key sign, with the shuck test, was positive. Hence, it was decided to address the DRUJ instability. With the forearm in the prone position, the incision was taken over the dorsal aspect of the wrist (Fig. 3). The 4th and the 5th extensor compartments were released and the tendons were elevated and retracted to expose the dorsal aspect of the DRUJ joint. The dorsal radioulnar ligament with surrounding soft tissue was found to be disrupted. Articular surfaces of the DRUJ were examined and were found to be healthy and amenable. to reconstruction Hence, the decision of DRUJ reconstruction was taken.
The wrist was placed in the supine position, and DRUJ was relocated and held in position temporarily with K-wire across the DRUJ. A fine guidewire was passed into the ulna from the ulnar to the radial aspect just proximal to DRUJ with the corresponding footprint marked on the medial aspect of the distal radius. The guidewire in the ulna was drilled over by the 4 mm cannulated drill bit to make an intraosseous tunnel around 5 mm proximal to DRUJ. The K-wire across the DRUJ was removed and the wrist was put into the prone position. A forearm Hohmann spike was introduced in between the radius and ulna just proximal to the DRUJ (around 5 mm) and placed on the radius levering down the ulna thus providing the exposure to the distal radius and reducing the distal ulna. The footprint marked earlier was identified and the cortex was drilled by 3.2 mm drill bit. A 5 mm double-loaded suture anchor was screwed into the metaphyseal part of the distal radius and stronghold was confirmed by gentle tugs on the threads (Fig. 4). The threads from the suture anchors were shuttled and retrieved out of the tunnel (Fig. 5).  An endo-button was passed along the threads and placed flush to the ulna. The knot was tied after supinating the wrist and securing the endo-button flush to the ulna at the end of the tunnel. Placement was confirmed fluoroscopically. Stability was checked. Reefing of the remnant of the dorsal capsule was done and the wound was then closed (Fig. 6). Post-operative X-ray was done showing a reduction of DRUJ (Fig. 7).
An endo-button was passed along the threads and placed flush to the ulna. The knot was tied after supinating the wrist and securing the endo-button flush to the ulna at the end of the tunnel. Placement was confirmed fluoroscopically. Stability was checked. Reefing of the remnant of the dorsal capsule was done and the wound was then closed (Fig. 6). Post-operative X-ray was done showing a reduction of DRUJ (Fig. 7).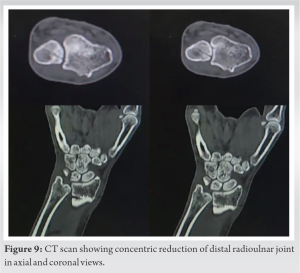
Post-operative rehabilitation
The patient was given above elbow slab for 6 weeks in a supine position with immediate start of active finger movements and shoulder movements. The wound healed uneventfully and suture removal was done on post-operative Day 12. The patient was then followed up every 2 weeks till 3 months from the surgery. After the removal of the slab at 6 weeks, the patient was started on wrist, forearm, and elbow mobilization. At 3-month follow-up, the patient had significant pain relief at the wrist joint and regained a painless and near-normal range of motion at the wrist joint. The patient has 80° of supination and 10° of pronation improving gradually. The grip of the patient went on to improve to near normal. Currently, the patient does not have any discomfort in continuing his job as a driver. The patient’s parameters improved significantly (Table 1).
Persistent instability of the DRUJ leads to an unfavorable result, with pain at the joint and restriction of forearm rotation. The goal of the treatment is an anatomic reduction and a rigid internal fixation of the radial fracture and restoration of normal anatomy of the DRUJ followed by intraoperative assessment of the DRUJ. Further, intraoperative interventions are based on the reducibility and post-reduction stability of the DRUJ. The ultrasonography of the DRUJ was done 3 months postoperatively and it showed the equal values of distance between the radius and ulna at DRUJ when compared to the opposite counterpart suggestive of appropriate reduction (Fig. 8). Post-operative CT scan confirmed concentric reduction of the DRUJ (Fig. 9). Extrinsic radioulnar tether was described by Fulkerson and Watson using a tendon graft looped around the neck of the ulna and threaded through the radius for the management of anterior dislocation of the distal ulna. It has recently been used for traumatic DRUJ instability also. The mean Quick-DASH and VAS were reduced significantly [5]. An article by Dy et al. states that the extensor retinaculum capsulorrhaphy or the Herbert sling procedure uses an ulnar-based flap of extensor retinaculum to stabilize the DRUJ. If imbrication of the extensor retinaculum is not performed in an oblique direction, the ulnocarpal effect of the sling is lost, and a supination deformity of the wrist may occur or reoccur. The Herbert sling repair can loosen if aggressive strengthening is undertaken too quickly; gentle active rotatory motion should only be introduced after an extended period of immobilization [6]. Hui and Linshead described the ulnocarpal sling procedure using a distally based strip of FCU tendon to reconstruct the volar ulnocarpal ligament. The repair also imbricates the dorsal radioulnar ligament upon itself, and the forearm is initially pinned in supination by a K-wire until ligament healing. Although all the patients had some loss of pronation, they were satisfied with the results of the operation. This procedure is most suitable for young, active patients with symptomatic subluxation of the DRUJ that is free from degenerative arthritis. Limitation of pronation was observed to be the most frequent complication of this procedure [7]. Brian Adams and Berger, in their article, stated that reconstruction of the volar and dorsal radioulnar ligaments has been described as anatomically reconstruct the dorsal and volar radioulnar ligaments and is often used with good results. All patients attained near-full pronation and supination [8]. Verhiel et al. stated resection of distal ulna (Darrach procedure) and Sauve–Kapandji procedures as the joint salvage procedures in arthritic changes. The author retrospectively analyzed 85 patients treated by either a Darrach (n = 57) or Sauvé–Kapandji procedure (n = 28). Complication and reoperation rates are relatively high, with non-significant differences between the two procedures [9]. TightRope is a relatively new technique for fixation. It comprises of a non-absorbable FiberWire held tight between two cortical metal buttons. As the TightRope provides semirigid fixation of syndesmosis, it obviates the need for routine removal of the implant and allows for early physical exercises [10]. The technique described in this paper has not been described before for the wrist in any available literature. As there is no use of tendon autograft in this technique, donor site morbidity and complications can be avoided. Lesser instrumentation is required as there is no need of autograft and can be practiced in setups with minimal requirements. It allows faster mobilization with earlier, better regain of range of motion, consumes lesser time with shorter learning curve, and similar or better outcome as compared to conventional techniques for DRUJ stabilization (Table 1).
Reconstruction of DRUJ using this novel technique provides good functional outcome including pain relief, improvement in hand grip and movements at the wrist and elbow joint similar to conventional techniques of intra as well as extra-articular tenodesis without causing donor site morbidity to the patient with lesser instrumentations and significantly reduced operating time. Although the outcome of this study is good, it is anecdotal evidence. More patients need to be operated with the same technique. Limitations of this study are that this technique has been done only in one patient, hence more patients need to be operated similarly. Furthermore, the longer follow-up is required to establish its efficacy. It requires an additional implant for fixation as compared to conventional techniques.
This novel new technique provides an effective treating option for chronic DRUJ instability without causing graft donor site morbidity for painless, functional mobilization of patients.
References
- 1.Nhamoucha Y, Tazi M, Alaoui O, Abdellaoui H, Atarraf K, Chater L, et al. Galeazzi fracture in children: About 5 cases and literature review. Pan Afr Med J 2018;30:274. [Google Scholar]
- 2.Johnson NP, Smolensky A. Galeazzi fractures. In: StatPearls. Treasure Island: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470188 [Last accessed on 2022 Jul 18]. [Google Scholar]
- 3.Perron AD, Hersh RE, Brady WJ, Keats TE. Orthopedic pitfalls in the ED: Galeazzi and monteggia fracture-dislocation. Am J Emerg Med 2001;19:225-8. [Google Scholar]
- 4.Bruckner JD, Alexander AH, Lichtman DM. Acute dislocations of the distal radioulnar joint. Instr Course Lect 1996;45:27-36. [Google Scholar]
- 5.Purisa H, Sezer I, Kabakas F, Tuncer S, Erturer E, Yazar M. Ligament reconstruction using the fulkerson-watson method to treat chronic isolated distal radioulnar joint instability: Short-term results. Acta Orthop Traumatol Turc 2011;45:168-74. [Google Scholar]
- 6.Dy CJ, Ouellette EA, Makowski AL. Extensor retinaculum capsulorrhaphy for ulnocarpal and distal radioulnar instability: The herbert sling. Tech Hand Up Extrem Surg 2009;13:19-22. [Google Scholar]
- 7.Hui FC, Linscheid RL. Ulnotriquetral augmentation tenodesis: A reconstructive procedure for dorsal subluxation of the distal radioulnar joint. J Hand Surg Am 1982;7:230-6. [Google Scholar]
- 8.Adams BD, Berger RA. An anatomic reconstruction of the distal radioulnar ligaments for posttraumatic distal radioulnar joint instability. J Hand Surg Am 2002;27:243-51. [Google Scholar]
- 9.Verhiel SH, Özkan S, Ritt MJ, Chen NC, Eberlin KR. A comparative study between darrach and sauvé-kapandji procedures for post-traumatic distal radioulnar joint dysfunction. HAND (N Y) 2021;16:375-84. [Google Scholar]
- 10.Zhang L, Xiong JX, Zhou X, Xiong LJ, Yu L. Biomechanical comparison of screw, tightrope and novel double endobutton in the treatment of tibiofibular syndesmotic injuries. Injury 2021;52:2813-9. [Google Scholar]








