This article describes a rare injury in adolescent sportsmen and women and the positive impact of different treatment methods on consolidation and return to sport
Dr. Muluem Olivier Kennedy, Yaounde General Hospital, BP: 5408, Yaounde. E-mail: kennedymuluem@yahoo.fr
Introduction: Tibial tubercle avulsion fractures are a rare lesion in adolescence that occurs during sports such as basketball, soccer, and volleyball. They result from a forceful extension of the knee against a fixed leg.
Case Report: Case 1: A 14-year-old adolescent who reportedly experienced severe knee pain when he jumped to head a ball during a soccer game. Case 2: A 17-year-old teenager who reportedly experienced severe knee pain on takeoff during a high jump event. Case 3: A 16-year-old who reportedly felt pain during takeoff to catch a basketball. Case 4: A 14-year-old adolescent who reportedly felt pain in his left knee on takeoff from a high jump during a basketball game. All of these patients presented with a defective leg extension on clinical examination. Radiographs showed an avulsion fracture of the anterior tibial tuberosity and treatment was surgical.
Discussion: Avulsion fractures of the tibial tuberosity are rare lesions. They occur in adolescents during sports and are usually accompanied by fracture fragment displacement, indicating reduction, and internal fixation surgery by screwing. In the short term, the result is satisfactory.
Conclusion: Tibial tuberosity avulsion fractures when managed in their entirety, give better results with a precocious return to sport.
Keywords: Avulsion fracture, tibial tuberosity, adolescent, sport.
Anterior tibial tuberosity (ATT) avulsion fractures are a rare injury that accounts for approximately 0.4–1.7% of all epiphyseal injuries [1]. They usually occur during recreational sports such as high jump, volleyball, basketball, and soccer, and are a source of disability [2]. They are often associated with a history of Osgood–Schlatter disease [3]. Treatment is surgical if the lesion is displaced and orthopedic in cases of non-displaced lesions [3]. We report four cases of tibial tubercle avulsion fractures that occurred in young adolescents during sports.
(Table 1)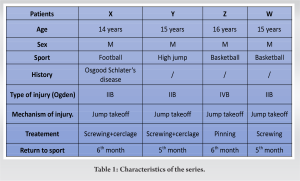
Case 1: Patient X
A 14-year-old soccer student presented with anterior knee pain, who reportedly experienced severe knee pain on takeoff to head a ball during a soccer game. This resulted in functional impairment of the limb. Physical examination revealed a sub-patellar notch and an impaired extensor function of the leg. Knee radiographs showed an avulsion fracture tibial tuberosity, classified Ogden Type IIB (Fig. 1a and b). The indication for open reduction and internal fixation (ORIF) was made and performed on the 2nd day of trauma. The approach was medial, and we performed a reduction and screwing of the fragments associated with a steel wire protection frame as cerclage (Fig. 1c and d). Removal of the cerclage wire was done on day 45 and consolidation was obtained at 2 months. Physiotherapy started 14 days after surgery. It consisted of muscular reinforcement by electrostimulation and passive mobilization up to 60° followed by active mobilization up to a range of 135° flexion and 0° extension after the removal of wire. The patient was able to resume sports at 6 months after removal of the screws.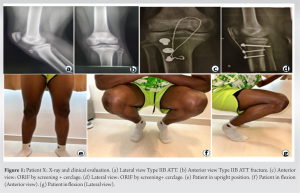
Case 2: Patient Y
A 17-year-old student who was practicing the high jump and experienced severe knee pain during take-off. Physical examination revealed a passive extension deficit of the leg. A radiograph of the knee showed an avulsion fracture, classified as Ogden Type IIB (Fig. 2a). Surgical intervention was indicated and we performed an ORIF by screw fixation with 2 cortical screws associated with a steel wire protection frame as cerclage (Fig. 2b and c). Healing was obtained on the 15th day, and rehabilitation was started immediately Quadriceps contraction by electrostimulation and passive followed by active mobilization of the knee. The cerclage wire was removed on day 90 and sports was resumed at 6 months’ post-operative.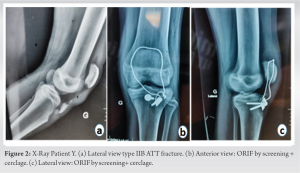
Case 3: Patient Z
A 16-year-old student reportedly experienced severe knee pain while catching a ball during a basketball game. Clinical examination revealed a partial extension deficit of the leg. An X-ray showed an avulsion fracture of the tibial tuberosity, classified Ogden Type IVB (Fig. 3a). A closed reduction and internal fixation (ORIF) by pinning was done under fluoroscopic guidance on day 2 of trauma (Fig. 3b). Immobilization by a rigid knee splint was done and rehabilitation by reinforcement of the quadriceps and mobilization of the knee began 45 days post-operation.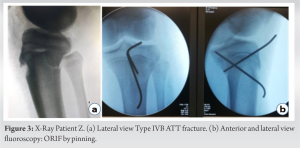
Case 4: Patient W
A 14-year-old student with no prior history reportedly experienced severe left knee pain on takeoff from a high jump during a basketball game. This resulted in absolute functional impairment of the limb. The physical examination revealed a defective extension of the left leg. An X-ray showed an avulsion fracture of the tibial tuberosity, classified as Ogden Type IIB (Fig. 4a and b). The indication for an ORIF by screw fixation was given and performed (Fig. 4c and d). Consolidation was obtained after 60 days and resumption of sports at 5 months.
It should be noted that all four patients each wore a rigid knee brace in knee extension for 3 weeks after surgery and walked with the aid of a pair of crutches for 2 months. Complete mobilization of the knee was obtained on the 3rd month for all four patients (Fig. 1e, f, g and 4e, f, g, h).
Tibial tuberosity avulsion fracture is a rare injury that usually occurs in adolescent males [4, 5]. High jump sports are the most incriminated in the genesis of these injuries as seen in basketball, soccer, volleyball, high jump, etc. [2]. Our four cases occurred in adolescent males during sports practice (soccer, high jump, and basketball). Indeed, during the practice of these sports, there is a sharp contraction of the quadriceps during knee extension while initiating a jump, which could lead to brutal traction on the tibial tuberosity, thus favoring its fracture by an avulsion [6, 7]. The association with Osgood–Schlatter disease is frequent [8]. In our study, only one patient (the 14-year-old) had a history of Osgood–shlatter’s disease with a history of chronic knee pain.
Watson Jones classified avulsion fractures of the tibial tuberosity into three types:
- Type I is an avulsion of a small portion of the tibial tuberosity, distal to the physis of the proximal tibia;
- Type II involves the whole physics, but does not extend to the knee joint;
- Type III corresponds to avulsion that extends proximally to the knee growth plate [9].
This classification was modified by Ogden and Southwick who added two other types corresponding to fragmentation and displacement of the fragment. Ryu and Debenham added a Type IV corresponding to the fracture of the ATT with a line that extends onto the posterior inferior metaphysis [10,11]. This type corresponds to an apophyseal detachment of the proximal tibia, Type II of Salter and Harris. Amongst our four patients, three presented with an Ogden’s Type IIB fracture and one with Type IVB.
Treatment is controversial in the literature. It can be non-operative or operative. The choice depends on the position of the fracture line and the displacement. For non-displaced fractures, orthopedic treatment can be performed. Type IA and IIA fractures can also be operated on with CRIF guided by fluoroscopy, followed by immobilization of the knee in extension for 6 weeks. Type IIB and III AB, on the other hand, are treated surgically from the start. Type IB can be treated by orthopedic management except in cases with periosteal interposition [11].
For other types (IA and rarely non-displaced Types II and III) they are treated by orthopedic management [12]. Type IV is treated surgically. Several means of fixation have been described: Pinning, screwing, and plating [13,14]. Some authors recommend a lateral approach to avoid transecting the infrapatellar nerve, which is a branch of the saphenous nerve. Other authors prefer a direct anterior approach, which allows for a better reduction of the fragments [5].
We performed surgery (open screwing of the fragments + protective frame by cerclage wiring) through the anterior approach in patients with Type IIB fractures and percutaneous pinning through the anterior approach under fluoroscopic guidance for the patient with Type IV fracture.
Intra- and post-operative complications have been described, including nerve damage, compartment syndrome due to traumatic section of the branches of the recurrent tibial artery, pulmonary embolism, calcification, and other complications, pulmonary embolism, vicious callus, and quadriceps atrophy. We did not record any complications in our patients.
At an average follow-up of 6 months, all four of our patients had resumed sports activity and the functional results were excellent. Our functional results are comparable to those reported in the literature.
TTA fracture is a rare injury that occurs most often in adolescent athletes. It is due to a sudden contraction of the quadriceps with the leg in extension. Several types are described depending on the location of the fracture line and the displacement. Whether the treatment is orthopedic or surgical, and when it is well conducted, the functional result is generally satisfactory with a return to sport within 6 months.
The avulsion fracture of the tibial tuberosity is a rare injury often occurring in adolescent athletes. Its treatment varies according to its severity. However, an early diagnosis and adequate management allow a return to sport at the same level.
References
- 1.Tourdias D, Hostyn V, Tourdias G. Avulsion fracture of the anterior tibial tuberosity in a young athlete. Ann Fr Med Urgence 2014;4:190. [Google Scholar]
- 2.Zaizi A, El Yaacoubi T, Chafry B, Boussouga M. Tibial tubercle avulsion fractures in school sports injury: A case report. Int J Surg Case Rep 2019;58:30-2. [Google Scholar]
- 3.Pesl T, Havranek P. Acute tibial tubercle avulsion fractures in children: Selective use of the closed reduction and internal fixation method. J Child Orthop 2008;2:353-6. [Google Scholar]
- 4.Pretell-Mazzini J, Kelly DM, Sawyer JR, Esteban EM, Spence DD, Warner WC Jr, et al. Outcomes and complications of tibial tubercle fractures in pediatric patients: A systematic review of the literature. J Pediatr Orthop 2016;36:440-6. [Google Scholar]
- 5.Da Silva Júnior AT, da Silva LJ, da Silva Filho UC, Teixeira EM, Araújo HR, de Moraes FB. Anterior avulsion fracture of the tibial tuberosity in adolescents-two case reports. Rev Bras Ortop 2016;51:610-3. [Google Scholar]
- 6.Bauer T, Milet A, Odent T, Padovani JP, Glorion C. Avulsion fracture of the tibial tubercle in adolescents: 22 cases and review of the literature. Rev Chir Orthop Reparatrice Appar Mot 2005;91:758-67. [Google Scholar]
- 7.Abalo A, Akakpo-Numado KG, Dossim A, Walla A, Gnassingbe K, Tekou AH. Avulsion fractures of the tibial tubercle. J Orthop Surg (Hong Kong) 2008;16:308-11. [Google Scholar]
- 8.Bombah FM, Nana T, Ekani BY, Biwole D, Handy E. Fracture-avulsion of tibial tubercle apophyseal in two Cameroonian adolescents. Trauma Case Rep 2021;35:100525. [Google Scholar]
- 9.Roy SP, Nag K. Simultaneous bilateral tibial tuberosity avulsion fractures in adolescence: Case report and review of 60 years of literature. Injury 2013;44:1953-5. [Google Scholar]
- 10.Watson-Jones R. Fractures and Joint Injuries. 4th ed. Baltimore: Williams and Wilkins; 1955. [Google Scholar]
- 11.Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res 1985;194:181-4. [Google Scholar]
- 12.Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ. Tibial tuberosity fractures in adolescents. J Child Orthop 2008;2:469-74. [Google Scholar]
- 13.Shelton WR, Canale ST. Fractures of the tibia through the proximal tibial epiphyseal cartilage. J Bone Joint Surg Am 1979;61:167-73. [Google Scholar]
- 14.Pace JL, McCulloch PC, Momoh EO, Nasreddine AY, Kocher MS. Operatively treated type IV tibial tubercle apophyseal fractures. J Pediatr Orthop 2013;33:791-6. [Google Scholar]