
Accessory EPL tendon can be initially missed on imaging. Knowledge of this anatomic variation allows the surgeon to anticipate this finding and plan accordingly to mitigate an iatrogenic injury.
Dr. Eagen Gene Deune, Department of Orthopaedic Spine Surgery, Boston University Medical Center, Boston, Massachusetts, USA. E-mail: eagen.deune@bmc.org
Introduction: Variations of the extensor pollicis longus (EPL) tendon of the hand are not uncommon. Yet, this anatomic structure exhibits the least variations among the extensors of the upper extremity.
Case Report: This article highlights the presence of an accessory EPL tendon in the fourth dorsal compartment, which was presented as an incidental finding during an elective wrist arthrodesis in a woman in her 40s.
Conclusion: Knowledge of this anatomic variation can guide surgical planning and mitigate iatrogenic injury by anticipating potential challenges.
Keywords: Extensor pollicis longus, anatomic variation, wrist arthrodesis.
Anatomic variations in the extensor compartments of the hand are not uncommon, including an accessory extensor pollicis longus (EPL) tendon with an anomalous course. According to the literature, the course of the EPL tendon passes through the third dorsal compartment and inserts dorsally at the base of the distal phalanx of the thumb1. There have been several reports describing different anatomic variations of the EPL tendon. However, this case describes a unique incidental finding of an accessory EPL tendon in the fourth dorsal compartment that became an obstacle during an elective wrist arthrodesis. Highlighting this anatomic variation and the surgical steps adopted in this report could help in future surgical planning and avoid iatrogenic damage to the tendon.
A right-handed female in her 40s with a history of intravenous (IV) drug use, Type 1 diabetes, and chronic kidney disease presented to the clinics with complaints of chronic right wrist pain and stiffness that started 6 months before presentation. Initially, the patient presented with a right distal forearm abscess, for which she received IV antibiotics followed by irrigation and debridement. On physical exam, the sensation of the hand and wrist was intact. The patient had localized tenderness over the carpal region and decreased range of motion on flexion, extension, radial, and ulnar deviation of the right wrist. The passive and active range of motion of the thumb did not elicit any pain. Radiographs of the right wrist revealed osteolysis and destructive erosive changes suggestive of osteomyelitis at the radiocarpal, intercarpal, and carpometacarpal regions. Pre-operative magnetic resonance imaging (MRI) of the wrist revealed extensive synovitis in similar anatomic regions. After failed conservative management, the patient was scheduled for radio carpometacarpal arthrodesis due to persistent pain and degenerative arthritis.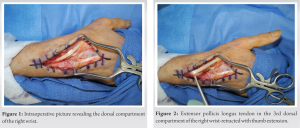
A dorsal longitudinal incision was performed along the third metacarpal axis and between the third and fourth dorsal extensor compartments. Starting from the Lister’s tubercle, the main EPL tendon was identified, released from the third dorsal compartment, and retracted radially (Figs. 1 and 2). Subsequently, a subperiosteal elevation of the fourth dorsal compartment was performed and reflected ulnarly to expose the radiocarpal joint. During this dissection, an accessory EPL tendon that extended the thumb at the interphalangeal (IP) joint, though not as strong as the main EPL, was incidentally identified (Fig. 3).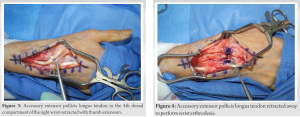 The supernumerary EPL tendon was approximately half the size of the main EPL tendon. The remaining neighboring tendons did not lead to a similar action of the EPL when tested, and traction of the accessory EPL tendon did not cause a simultaneous extension of the index finger. Because the accessory EPL tendon crossed the surgical field from the fourth dorsal compartment radially to the thumb’s distal phalanx, careful ulnar retraction was required to avoid tendon injury (Fig. 4). Furthermore, an additional extension of the incision proximally and distally was required to allow for adequate retraction of the accessory EPL tendon and proper fusion plate placement. Once the bony surfaces of the radius, carpus, and third metacarpal bones were prepared, a prevent short wrist fusion plate from the Integra (Smith and Nephew) Wrist Fusion system was installed. The plate was fixed distally to the third metacarpal and proximally to the distal dorsal radius. During this step, Ragnell retractors were used to prevent injury to the accessory EPL. Before the incision closure, the accessory EPL tendon was left superimposed over the fusion plate with an intervening soft-tissue layer in between.
The supernumerary EPL tendon was approximately half the size of the main EPL tendon. The remaining neighboring tendons did not lead to a similar action of the EPL when tested, and traction of the accessory EPL tendon did not cause a simultaneous extension of the index finger. Because the accessory EPL tendon crossed the surgical field from the fourth dorsal compartment radially to the thumb’s distal phalanx, careful ulnar retraction was required to avoid tendon injury (Fig. 4). Furthermore, an additional extension of the incision proximally and distally was required to allow for adequate retraction of the accessory EPL tendon and proper fusion plate placement. Once the bony surfaces of the radius, carpus, and third metacarpal bones were prepared, a prevent short wrist fusion plate from the Integra (Smith and Nephew) Wrist Fusion system was installed. The plate was fixed distally to the third metacarpal and proximally to the distal dorsal radius. During this step, Ragnell retractors were used to prevent injury to the accessory EPL. Before the incision closure, the accessory EPL tendon was left superimposed over the fusion plate with an intervening soft-tissue layer in between.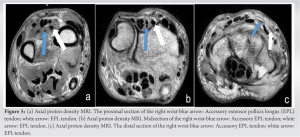 Because of time and exposure limitations during surgery, a separate muscle belly for the accessory EPL was visualized yet the muscle origin could not be identified. On the other hand, the insertion was inferred to be on the thumb distal phalanx based on intraoperative mechanical testing. The pre-operative MRI was reviewed again in light of this intraoperative finding to locate the accessory EPL (Fig. 5). Postoperatively, the wrist was placed in a short arm fiberglass cast for 4 weeks. It was transitioned to a custom occupational therapy splint for another 4 weeks while increasing the range of motion and daily activities. At her final follow-up (6 months), the patient recovered uneventfully with a healed incision, resolution of pain, and satisfying range of motion at the MCP, PIP, and DIP finger joints (Fig. 6).
Because of time and exposure limitations during surgery, a separate muscle belly for the accessory EPL was visualized yet the muscle origin could not be identified. On the other hand, the insertion was inferred to be on the thumb distal phalanx based on intraoperative mechanical testing. The pre-operative MRI was reviewed again in light of this intraoperative finding to locate the accessory EPL (Fig. 5). Postoperatively, the wrist was placed in a short arm fiberglass cast for 4 weeks. It was transitioned to a custom occupational therapy splint for another 4 weeks while increasing the range of motion and daily activities. At her final follow-up (6 months), the patient recovered uneventfully with a healed incision, resolution of pain, and satisfying range of motion at the MCP, PIP, and DIP finger joints (Fig. 6).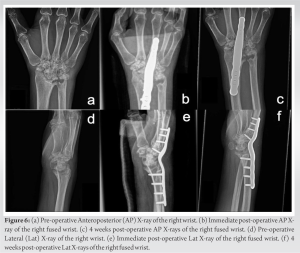
Usually, the EPL tendon runs its ordinary course in the third dorsal extensor compartment as the only tendon and allows for thumb extension. The posterior interosseous branch of the radial nerve innervates the EPL. It originates from the interosseous membrane and inserts on the distal phalanx of the thumb [1]. A supernumerary EPL tendon is an accessory or duplicated tendon. Yoshida reported that the EPL tendon is the most stable extensor tendon of the upper limb, with 3.6% of the cadaveric subjects having duplicated EPL tendons. The most common variation of the EPL tendon cited in the literature is based on the duplication of the tendon from the same or different muscle bellies of the EPL. Türker et al. described a classification system based on accessory tendons: Type 1 describes distinct tendons, while Type 2 describes tendon interconnections [2]. Previous case reports based on elective surgeries could not carry out extensive dissections to identify the EPL origin and insertion. Nevertheless, they classified their case as Type 1a according to the extension of the IP joint of the thumb following intraoperative traction of the accessory EPL tendon [2, 3, 4, 5]. Based on this classification, our case can be described as Type 1a.
In this case, the patient was unaware of this variation as they did not experience any symptoms or functional differences related to the accessory EPL tendon. Talbot mentioned that most anomalies related to muscle or tendon insertions duplicated or enhanced their function instead of altering it by presenting a new geometry of muscular function. He went on to describe that these individuals have no reference to comparing this functional enhancement to others [6]. As a result, these anatomic variations are mostly discovered incidentally. This report summarizes the types of accessory EPL tendons found incidentally during surgical cases or cadaveric dissections (Table 1). The incidental finding in our case became an obstacle when the accessory EPL tendon obstructed the plate’s insertion site. This is not the first case of a supernumerary EPL tendon running in the fourth dorsal compartment. De Greef reported a case with a similar incidental finding requiring a wrist arthrodesis [4]. However, it did not include a description of the intraoperative steps. This case report provides surgical steps required to handle an accessory EPL tendon following an intraoperative incidental finding. Knowledge of anatomy and its variation is crucial to allow preservation of the accessory tendon instead of being removed/cut to minimize any chance of adhesion or discomfort that may arise over the plate. Furthermore, the accessory tendon was left intact to preserve its function. For instance, in a report describing a full EPL tendon rupture following a distal radius fracture, the patient could extend their distal thumb phalanx, albeit to a lesser extent, due to the accessory EPL tendon [7]. Another advantage would be to use this accessory tendon as a graft in light of a tendon rupture repair.
The majority of the EPL tendon variants are due to the presence of an accessory tendon. Although these variations are asymptomatic and found incidentally, knowledge of their occurrence will guide surgical planning and help overcome intraoperative challenges.
The primary aim in documenting and sharing this case is to contribute to the ongoing scientific discourse about the human anatomical variations of the EPL and their impact on surgical practice. This anatomic variation can go unnoticed in imaging in the beginning. This report could be an important resource for surgeons who might encounter similar variations in the future, enabling them to plan their procedures better and anticipate potential challenges.
References
- 1.Yoshida Y. Anatomical study on the extensor digitorum profundus muscle in the Japanese. Okajimas Folia Anat Jpn 1990;66:339-53. [Google Scholar]
- 2.Türker T, Robertson GA, Thirkannad SM. A classification system for anomalies of the extensor pollicis longus. Hand (N Y) 2010;5:403-7. [Google Scholar]
- 3.Cohen BE, Haber JL. Supernumerary extensor tendon to the thumb: A case report. Ann Plast Surg 1996;36:105-7. [Google Scholar]
- 4.De Greef I, De Smet L. Accessory extensor pollicis longus: A case report. Eur J Plast Surg 2006;28:532-3. [Google Scholar]
- 5.Tordjman D, Pierrart J, Bellity J, Delgrande D, Masmejean E. Accessory extensor pollicis longus: A rare tendon anomaly. Hand Surg Rehabil 2018;37:60-3. [Google Scholar]
- 6.Talbot CE, Mollman KA, Perez NM, Zimmerman AM, Drew N, Tsung I, et al. Anomalies of the extensor pollicis longus and extensor indicis muscles in two cadaveric cases. Hand (N Y) 2013;8:469-72. [Google Scholar]
- 7.Wiekrykas BD, Solarz MK, Abdelfattah HM, Thoder JJ. Supernumerary extensor pollicis longus tendon masking an extensor pollicis longus rupture following non-surgical treatment of a distal radius fracture. BMJ Case Rep 2021;14:e242509. [Google Scholar]
- 8.Wood J. IV. Variations in human myology observed during the Winter session of 1866-67 at King’s college, London. Proc Royal Soc London 1867;15:518-46. [Google Scholar]
- 9.Kaplan EB, Nathan P. Accessory extensor pollicis longus. Bull Hosp Joint Dis 1969;30:203-7. [Google Scholar]
- 10.Chiu DT. Supernumerary extensor tendon to the thumb: A report on a rare anatomic variation. Plast Reconstr Surg 1981;68:937-9. [Google Scholar]
- 11.Culver JE Jr. Extensor pollicis and indicis communis tendon: A rare anatomic variation revisited. J Hand Surg Am 1980;5:548-9. [Google Scholar]
- 12.Abu-Hijleh MF. Extensor pollicis tertius: An additional extensor muscle to the thumb. 1993;92:340-3 . [Google Scholar]
- 13.Papaloïzos MY. Accessory extensor pollicis longus. Scand J Plast Reconstr Surg Hand Surg 2004;38:310-3. [Google Scholar]
- 14.Beatty JD, Remedios D, McCullough CJ. An accessory extensor tendon of the thumb as a cause of dorsal wrist pain. J Hand Surg Br 2000;25:110-1. [Google Scholar]
- 15.Sawaizumi T, Nanno M, Ito H. Supernumerary extensor pollicis longus tendon: A case report. J Hand Surg 2003;28:1014-7. [Google Scholar]
- 16.Jiang Q, Zhou H, Huang K, Lu H. Accessory extensor pollicis longus tendon in emergency surgery. J Int Med Res 2020;48:1-5. [Google Scholar]
- 17.Bluth BE, Wu B, Elena Stark M, Wisco JJ. Variant of the extensor pollicis tertius: A case report on a unique extensor muscle to the thumb. Anat Sci Int 2011;86:160-3. [Google Scholar]
- 18.Nishijo K, Kotani H, Miki T, Senzoku F, Ueo T. Unusual course of the extensor pollicis longus tendon associated with tenosynovitis, presenting as de Quervain disease--a case report. Acta Orthop Scand 2000;71:426-8. [Google Scholar]
- 19.Sevivas N, Kalouche I, Roulot E. Double extensor pollicis longus tendon in independent extensor compartments: A case report of an anatomical variation requiring alteration of surgical strategy. Chir Main 2009;28:180-2. [Google Scholar]
- 20.Masada K, Yasuda M, Takeuchi E, Mizusawa K. Duplicate extensor tendons of the thumb mimicking rupture of the extensor pollicis longus tendon. Scand J Plast Reconstr Surg Hand Surg 2003;37:318-9. [Google Scholar]






