
This article showcases a rare case of an aneurysmal bone cyst (ABC) in the 3rd metatarsal, underscoring the need to recognize atypical foot swellings; surgical excision with fibular strut graft integration effectively resolved the lesion, emphasizing the vital role of thorough radiological and histological assessments for precise diagnosis and management.
Dr. Mainak Roy, Department of Orthopaedics, All India Institute of Medical Sciences, Nagpur, Maharashtra, India. E-mail: mainakroy30@gmail.com
Introduction: An aneurysmal bone cyst (ABC) is an unusual, non-cancerous bone lesion that is characterized by its lytic (causing bone loss), hemorrhagic, and expanding nature. ABCs are relatively rare, making up only 1% of all bone tumors. These cysts are typically found in long bones and the spine but are very rarely seen in the metatarsal bones, making such occurrences quite uncommon.
Case Report: In this case report, we present a case of ABC of the 3rd metatarsal in a 26-year-old female with complaints of long-standing foot pain and gradually increasing swelling of the dorsum of the foot. After radiological evaluation, she had undergone histopathological evaluation. An en bloc resection of the metatarsal along with the tumor mass was performed and the gap was replaced with an ipsilateral fibular strut graft. Histopathological examination of the resected tissue was suggestive of ABC without any evidence of malignancy. At the end of 1 year of follow-up, she is now completely pain free with intact rom of foot and ankle.
Conclusion: The present study aims to describe a case of ABC of the metatarsal, a condition that not only poses a diagnostic dilemma but also constitutes a challenge in the management of lesion.
Keywords: Aneurysmal bone cyst, metatarsal bone, foot swelling.
An aneurysmal bone cyst (ABC) is a non-cancerous, locally destructive bone abnormality that can occur as either a primary condition in about 79% of cases or as a secondary condition resulting from other bone conditions in approximately 20% of cases [1]. It typically affects individuals below the age of 20 years, with around 95% of cases occurring within the first three decades of life [2]. ABCs are relatively rare, constituting only about 1% of all bone tumors [3]. While ABCs can affect any bone in the body, they most commonly appear in the metaphysis (the growing part of the bone) of long bones (about 65% of cases), the pelvis (12%), and the spinal arch (12%) [4]. Only 7% of the ABCs are located in the metatarsal bones [3]. When diagnosing ABCs, it is important to differentiate them from other conditions such as giant cell tumors (GCTs), giant cell reparative granulomas (GCRGs), and brown tumors that can be associated with hyperparathyroidism [5]. Treatment options for ABCs include procedures such as autogenous bone grafting (using the patient’s bone tissue), cementation, or surgical removal of the lesion [6]. The present study discusses a rare case of an ABC localized in the metatarsal bone, which is an uncommon presentation. Only a few such cases have been reported in the medical literature to date.
A 26-year-old female presented with complaints of gradually increasing swelling over the dorsum of her right foot for the past 2 years (Fig. 1). There was no history of trauma or associated symptoms of fever or weight loss. It was a small swelling to start with but gradually progressed over the course of time. Initially, she was evaluated with an X-ray and was treated with some medication and sclerosant injection into the swelling elsewhere but there was no improvement in her symptoms. She then presented to our hospital with swelling over the dorsum of her foot, pain, and no other systemic complaints. The pain was aggravated by walking and activity. Swelling was mostly over the dorsum of the foot without any local signs of inflammation. She was evaluated by sending her blood samples and radiologically with the help of X-rays and magnetic resonance imaging (MRI). All the hematological parameters were within normal limits. The X-ray showed an expansile lytic destructive lesion involving the 3rd metatarsal with significant thinning of the cortex and septations without any calcification (Fig. 2). An MRI revealed an expansile bone lesion with multiple septations in the diaphysis of the right third metatarsal bone. This lesion was hypointense in T1 and hyperintense in T2-weighted images, along with the cortical breach in the ventral aspect of the third metatarsus. A core-needle biopsy under C-arm guidance was performed as per protocol for confirmation of diagnosis and prognostication of disease, and the sample was sent for histopathological evaluation. Under microscopy, there were large areas of hemorrhage with fibro-collagenous tissue and many giant cells with scattered hemosiderin-laden macrophages, which were suggestive of ABC. Surgical excision with autogenous fibular bone grafting was planned for the patient. A 10 cm linear incision was given in line with the third metatarsal and with the biopsy site. Skin and subcutaneous tissue were incised until the periosteum was reached. The periosteum was also incised in the line of the metatarsal and everted to expose the tumor mass. The tumor mass was exposed from all sides, and en bloc resection of the metatarsal was done (Fig. 3).
There was no history of trauma or associated symptoms of fever or weight loss. It was a small swelling to start with but gradually progressed over the course of time. Initially, she was evaluated with an X-ray and was treated with some medication and sclerosant injection into the swelling elsewhere but there was no improvement in her symptoms. She then presented to our hospital with swelling over the dorsum of her foot, pain, and no other systemic complaints. The pain was aggravated by walking and activity. Swelling was mostly over the dorsum of the foot without any local signs of inflammation. She was evaluated by sending her blood samples and radiologically with the help of X-rays and magnetic resonance imaging (MRI). All the hematological parameters were within normal limits. The X-ray showed an expansile lytic destructive lesion involving the 3rd metatarsal with significant thinning of the cortex and septations without any calcification (Fig. 2). An MRI revealed an expansile bone lesion with multiple septations in the diaphysis of the right third metatarsal bone. This lesion was hypointense in T1 and hyperintense in T2-weighted images, along with the cortical breach in the ventral aspect of the third metatarsus. A core-needle biopsy under C-arm guidance was performed as per protocol for confirmation of diagnosis and prognostication of disease, and the sample was sent for histopathological evaluation. Under microscopy, there were large areas of hemorrhage with fibro-collagenous tissue and many giant cells with scattered hemosiderin-laden macrophages, which were suggestive of ABC. Surgical excision with autogenous fibular bone grafting was planned for the patient. A 10 cm linear incision was given in line with the third metatarsal and with the biopsy site. Skin and subcutaneous tissue were incised until the periosteum was reached. The periosteum was also incised in the line of the metatarsal and everted to expose the tumor mass. The tumor mass was exposed from all sides, and en bloc resection of the metatarsal was done (Fig. 3). The wound was debrided thoroughly. The size of the metatarsal was measured, and an ipsilateral fibular graft was harvested. The graft was interposed and fixed with the tarsal bone proximally with a 3.5 recon plate and distally to the proximal phalanx with K-wire. The excised mass was then sent for histopathological examination. On histological examination, the lesion displayed non-cancerous reactive tissue characterized by a fibrohistiocytic framework, numerous multi-nucleated giant cells, and reactive bone encircling blood-filled gaps. There were no indications of dividing cells or abnormal cell nuclei, and these findings strongly indicated the presence of an ABC (Fig. 4).
The wound was debrided thoroughly. The size of the metatarsal was measured, and an ipsilateral fibular graft was harvested. The graft was interposed and fixed with the tarsal bone proximally with a 3.5 recon plate and distally to the proximal phalanx with K-wire. The excised mass was then sent for histopathological examination. On histological examination, the lesion displayed non-cancerous reactive tissue characterized by a fibrohistiocytic framework, numerous multi-nucleated giant cells, and reactive bone encircling blood-filled gaps. There were no indications of dividing cells or abnormal cell nuclei, and these findings strongly indicated the presence of an ABC (Fig. 4).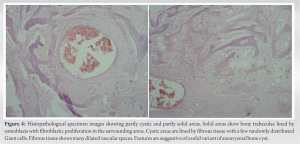 Hemostasis was maintained, and the wound was closed in layers. The foot was immobilized with plaster for 12 weeks. For the initial period of 3 weeks, slab support was applied. After suture removal, the slab was changed to a cast. Follow-up was done at 6 weeks, 3 months, 6 months, 1 year, and 2 years. The K-wire was removed at the end of 3 months, and she was allowed to bear partial weight. At the 2-year follow-up, the patient was completely pain-free and walking comfortably without any local swelling or wound complications. A 2-year follow-up X-ray (Fig. 5) showed that the graft was incorporated satisfactorily and with good consolidation. There were no signs of recurrence, either clinically or radiologically. The incorporation of a fibula graft filled the void left after the resection of the tumor mass, helped in the good cosmetic outcome, and also prevented a collapse of the third ray of her foot.
Hemostasis was maintained, and the wound was closed in layers. The foot was immobilized with plaster for 12 weeks. For the initial period of 3 weeks, slab support was applied. After suture removal, the slab was changed to a cast. Follow-up was done at 6 weeks, 3 months, 6 months, 1 year, and 2 years. The K-wire was removed at the end of 3 months, and she was allowed to bear partial weight. At the 2-year follow-up, the patient was completely pain-free and walking comfortably without any local swelling or wound complications. A 2-year follow-up X-ray (Fig. 5) showed that the graft was incorporated satisfactorily and with good consolidation. There were no signs of recurrence, either clinically or radiologically. The incorporation of a fibula graft filled the void left after the resection of the tumor mass, helped in the good cosmetic outcome, and also prevented a collapse of the third ray of her foot.
ABCs make up about 1% of all primary bone lesions that undergo biopsy [7]. While the exact cause of ABCs is not fully understood, the most widely accepted theory suggests that they result from disruptions in local blood circulation, leading to increased pressure in veins and the development of enlarged and dilated blood vessels within the affected bone [8]. It is crucial to differentiate between ABCs and other bone tumors containing giant cells, such as GCT, GCRG, and brown tumors [9]. GCTs consist of mononuclear and osteoclast-like multinucleated giant cells and can be locally aggressive. They are typically found in the epiphysis and metaphysis of bones, causing lytic expansion [10]. GCRG is a rare benign lesion characterized by a predominance of giant and mononuclear cells in areas of bleeding [11]. Brown tumors are associated with chronic renal deficiency and have a more lobulated architectural growth pattern. They can be distinguished from ABCs through serum calcium, parathyroid, and phosphorus hormone level testing [12]. In contrast, ABCs are histologically characterized by blood-filled cystic spaces separated by fibrous septae [9]. Computed tomography and MRI scans are helpful for diagnosing ABCs, with T2-weighted MRI being particularly useful for detecting the segmented, expansile, multiseptated lesion filled with fluid within the affected bone [13]. Surgical removal is the preferred treatment for ABCs. This involves removing the lesion through intralesional curettage using a wide cortical window, with the possibility of using allograft bone grafting to replace bone defects [14]. Embolotherapy has also been successful in treating ABCs [15]. However, it is important to inform patients that ABCs have a high recurrence rate, necessitating close monitoring for any signs of recurrence or malignant transformation [16].
In summary, ABC is a destructive and hemorrhagic lesion that mainly affects teenagers. While radiographs and MRI scans can aid in diagnosis, accurate histological evaluation is crucial. Treatments such as wide local excision and bone grafting are considered safe. There can be several other causes of swelling in the foot. Metatarsal ABCs should also be kept in mind while evaluating such cases and managed accordingly. Metatarsal ABCs tend to have a high recurrence and so long-term regular follow-up both clinically and radiologically is important to detect the lesion early.
This case underscores the diagnostic challenge posed by ABCs in atypical locations such as metatarsals, necessitating thorough radiological and histopathological assessments. Successful management involves en bloc resection and incorporation of fibular strut graft. The incorporation of fibular graft restores the biomechanics of the foot, prevents the collapsing of the third ray, and also aids in cosmesis. For smaller lesions simple extended curettage may suffice but for larger lesions bone grafting is usually needed to fill the void post-excision. Patients are to be kept on long-term regular follow-ups as ABCs have high recurrence rates.
References
- 1.Lichtenstein L. Aneurysmal bone cyst; further observations. Cancer 1953;6:1228-37. [Google Scholar]
- 2.Singh DK, Singh N, Pant MC. Aneurysmal bone cyst: An unusual presentation of back pain. Asian J Neurosurg 2014;9:105-7. [Google Scholar]
- 3.Hakim DN, Pelly T, Kulendran M, Caris JA. Benign tumours of the bone: A review. J Bone Oncol 2015;4:37-41. [Google Scholar]
- 4.Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop 1986;204:25-36. [Google Scholar]
- 5.Barnhart MD. Malignant transformation of an aneurysmal bone cyst in a dog. Vet Surg 2002;31:519-24. [Google Scholar]
- 6.Ozaki T, Hillmann A, Lindner N, Winkelmann W. Aneurysmal bone cysts in children. J Cancer Res Clin Oncol 1996;122:767-9. [Google Scholar]
- 7.Freiberg AA, Loder RT, Heidelberger KP, Hensinger RN. Aneurysmal bone cysts in young children. J Pediatr Orthop 1994;14:86-91. [Google Scholar]
- 8.Brindley GW, Greene JF Jr., Frankel LS. Case reports: Malignant transformation of aneurysmal bone cysts. Clin Orthop 2005;438:282-7. [Google Scholar]
- 9.Gibbs CP Jr., Hefele MC, Peabody TD, Montag AG, Aithal V, Simon MA. Aneurysmal bone cyst of the extremities. Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-8. [Google Scholar]
- 10.Tumours and Tumour-Like Lesions in the Foot and Ankle. Available from: https://pubmed.ncbi.nlm.nih.gov/15710135 [Last accessed on 2023 Sep 28]. [Google Scholar]
- 11.Cook DL, Rosenthal DC, Shikoff MD. Giant cell reparative granuloma of the middle phalanx of the foot: A review and case report. J Foot Ankle Surg 2008;47:589-93. [Google Scholar]
- 12.Hanna BG, Donthineni R, Majid K, Parekh S, Shin JS, Lackman RD. Leg mass in a 61-year-old man. Clin Orthop 2003;406:298-307. [Google Scholar]
- 13.Iltar S, Alemdaroğlu KB, Karalezli N, Irgit K, Caydere M, Aydoğan NH. A case of an aneurysmal bone cyst of a metatarsal: Review of the differential diagnosis and treatment options. J Foot Ankle Surg 2009;48:74-9. [Google Scholar]
- 14.Boubbou M, Atarraf K, Chater L, Afifi A, Tizniti S. Aneurysmal bone cyst primary--about eight pediatric cases: Radiological aspects and review of the literature. Pan Afr Med J 2013;15:111. [Google Scholar]
- 15.Rastogi S, Varshney MK, Trikha V, Khan SA, Choudhury B, Safaya R. Treatment of aneurysmal bone cysts with percutaneous sclerotherapy using polidocanol. A review of 72 cases with long-term follow-up. J Bone Joint Surg Br 2006;88:1212-6. [Google Scholar]
- 16.Cugati G, Pande A, Jain PK, Symss NP, Ramamurthi R, Vasudevan CM. Aneurysmal bone cyst of the lumbar spine. Asian J Neurosurg 2015;10:216-8. [Google Scholar]








