
These two cases of delayed union biphalangeal toe fractures showed the possibility of undergoing surgical fixation in cases of long-term pain.
Akihiro Itamoto, Department of Orthopaedic Surgery, Graduate School of Medicine, Kyoto University, 54 Kawahara-cho, Shogoin, Sakyo-ku, Kyoto, 606-8507, Japan. E-mail: a_itamoto1@kuhp.kyoto-u.ac.jp
Introduction: The prognosis for toe fractures with coalition is generally good, but in some cases, bone union may not be achieved. This is the report in which good results are obtained by surgery for a painful delayed union of biphalangeal toe fractures.
Case Report: Case 1: A 64-year-old Japanese woman had left toe pain for 7 months. Plain radiography showed fourth toe fracture with coalition. Surgical fixation was performed. Case 2: A 63-year-old Japanese woman had left toe pain for a month. Plain radiography showed third toe fracture with coalition. No improvement was achieved with conservative treatment, and surgical treatment was performed.
Conclusion: Surgical treatment should be performed for the nonunion of symphalangistic distal phalanx fractures with long-term pain.
Keywords: Biphalangeal toe, toe fracture, delayed union, symphalangism.
Toe symphalangism is a congenital segmental insufficiency of the distal and intermediate phalanxes, which is present in 37–40% of Caucasians and 73% of Japanese [1]. Bone union of toe fractures with coalition is generally successful; however, there are some reports of prolonged healing and non-union cases in biphalangeal toe fractures. Few reports have documented cases of surgical fixation for fused toe fractures. Here, two cases of surgery for delayed union of a toe fracture with symphalangism are reported.
Case 1
History
A 64-year-old woman injured her left toe 7 months before the first visit to our hospital, and suffered from persistent pain and swelling in the left fourth toe. The patient experienced both resting and walking pain.
Examination
Swelling and tenderness in the left fourth toe segment were observed.
Radiography
A fracture at the fusion site between the left distal and intermediate phalanxes observed (Fig. 1a). Computed tomography (CT) revealed poor callus formation (Fig. 1b). Surgical fixation was selected as the treatment, as the symptoms were long-standing.
Operation
Refreshment of the fracture area was performed through a lateral approach to the nonunion site using a K-wire and a sharp curette. Subsequently, a guide wire was inserted and a cannulated headless compression screw (Acutrak 2 Micro, Acumed, Portland, OR, USA) was inserted in the apex of the toe to crimp the bone fragment using it as a guide, and the proximal interphalangeal (PIP) joint was fixed using a K-wire inserted at the apex of the toe and passing through the joint (Fig. 1c). The pain was relieved immediately after the operation. One week after the operation, the K-wire was removed and the patient wore a forefoot splint and was allowed to walk under load. The forefoot splint was removed 6 weeks after surgery. The patient exhibited bone fusion 6 months after surgery (Fig. 1d). The patient’s resting and walking pain improved dramatically, and she was able to stand on her toes.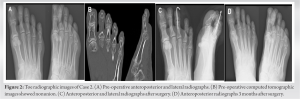
Case 2
History
A 63-year-old woman fell a month before the first visit to our hospital and consulted a local doctor for persistent pain and swelling in her right third toe. The patient was treated conservatively but was referred to our hospital because she remained symptomatic.
Examination
The patient experienced walking pain and had difficulty loading her forefoot. Physical examination revealed swelling and tenderness in the distal phalanx of the right third toe.
Radiography
Delayed union of the symphalangistic distal phalanx fracture was observed (Fig. 2a). CT revealed poor callus formation (Fig. 2b). Initially, non-operative therapy using a cast was performed, but the union was delayed, and the pain persisted; therefore, surgery was planned 3 months after the initial trauma.
Operation
Refreshment of the fracture area was performed through a lateral incision. The PIP joint was fixed using a K-wire inserted at the toe apex and through the joint (Fig. 2c). Post-operative cast fixation was applied 7 weeks after surgery, the K-wire was removed, and the cast fixation was removed. Bone fusion was achieved 3 months after the operation (Fig. 2d), and forefoot loading was possible without pain.
Here, we report two cases of delayed union of a symphalangistic distal phalanx fracture. Conservative treatment was performed; however, the pain persisted, and surgical treatment was performed, yielding bone union and pain relief. The frequency of toe coalition in Japanese individuals is 72.5% for the 5th toe, 11.9% for the 4th toe, 0.8% for the 3rd toe, and 0.0% for the 2nd toe [2]. Fifth toe fusion is bilateral in 88–94% of cases [3] and there are no differences between sexes and the left or right [2, 4-6]. A fracture at the fusion site between the distal and the middle phalanges tends to result in prolonged bone fusion [7]. The reasons for this include increased stress caused by the stiffness of the toe and the longer lever arm at the fused site, insufficient external fixation, early loading, and mistaking a fracture for a normal joint when the radiographic image is insufficient [7]. Toe fractures without coalition are mainly treated using stiff-sole shoes and buddy taping and often heal within approximately 4–6 weeks [8]. Biphalangeal toe fractures are typically pain-free, even if union is not obtained; therefore, conservative treatments such as buddy taping and cast fixation are recommended [7]. Few reports document surgeries for symphalangistic toe fractures; one reported PIP joint fixation being performed, in cases of painful nonunion in the fourth toe, using a cannulated compression headless screw [9]. In terms of the operative procedure, a previous study comparing K-wire and screw fixations for distal phalangeal fractures did not show a significant difference in bone fusion [10], and there was no clear evidence of which method is better. In both of the current cases, union could not be achieved despite a long period of conservative treatment, pain persisted, and surgery was performed. Pain was improved and bone fusion was achieved using the screw and wire together or the wire alone, suggesting that surgical treatment may be required for patients with long-term pain due to bone nonunion.
Two cases are presented with improved pain after surgery for delayed union of biphalangeal toe fractures with prolonged pain. We suggest that surgical treatment should be performed for the nonunion of symphalangistic distal phalanx fractures with long-term pain.
These cases highlight that surgical intervention is crucial for painful delayed union of biphalangeal toe fractures with coalition. The positive outcomes emphasize the efficacy of surgical fixation in resolving long-term pain. We should consider timely surgical treatment in cases of non-union for improved patient outcomes.
References
- 1.Keats TE. Atlas of Normal Roentgen Variants that May Simulate Disease. 9th ed. Philadelphia, PA: Saunders; 2012. p. 702-3. [Google Scholar]
- 2.Nakashima T, Hojo T, Suzuki K, Ijichi M. Symphalangism (two phalanges) in the digits of the Japanese foot. Ann Anat 1995;177:275-8. [Google Scholar]
- 3.Thompson FM, Chang VK. The two-boned fifth toe: Clinical implications. Foot Ankle Int 1995;16:34-6. [Google Scholar]
- 4.Case DT, Heilman J. Pedal symphalangism in modern American and Japanese skeletons. Homo 2005;55:251-62. [Google Scholar]
- 5.Dereymaeker G, van der Broek C. Biphalangeal fifth toe. Foot Ankle Int 2006;27:948-51. [Google Scholar]
- 6.Ceynowa M, Rocławski M, Pankowski R, Mazurek T. The prevalence and ossification pattern of the biphalangeal and triphalangeal lateral toes. Surg Radiol Anat 2018;40:1039-1045. [Google Scholar]
- 7.Sammarco GJ, Hockenbury RT. Fracture of an interphalangeal coalition: A report of two cases. Foot Ankle Int 2000;21:690-2. [Google Scholar]
- 8.Bica D, Sprouse RA, Armen J. Diagnosis and management of common foot fractures. Am Fam Physician 2016;93:183-91. [Google Scholar]
- 9.Foo GL, Wee L. Surgical fixation and inter-phalangeal arthrodesis of symptomatic non-union of fracture of a lesser toe distal phalanx: A case report. Malays Orthop J 2019;13:69-71. [Google Scholar]
- 10.Hay RA, Tay SC. A Comparison of K-wire versus screw fixation on the outcomes of distal phalanx fractures. J Hand Surg Am 2015;40:2160-7. [Google Scholar]




