Time-saving and cost-effective solution for closure of horizontal cleavage tears of the meniscus.
Dr. Hitendra G Patil, Pimprikar Hospital, Chowk no 5, Govind Nagar, Nashik - 422 009, Maharashtra, India. E-mail: drhitendrapatil@gmail.com
Introduction: Horizontal cleavage tears (HCT) of the meniscus are treated with fish-mouth closure with sutures using different methods. Using a no. 0 fiber wire and taking bites through both the flaps using a suture passing device and tying multiple knots is a cost-effective technique. A racking hitch knot is an option for all inside repairs of HCT. It needs multiple half hitches for locking the knot.
Surgical Technique: We used a modification of the racking hitch knot (HP knot), making it a self-locking knot, so it does not need half hitches. Loop of no. 0 fiber wire is passed across both the flaps of the meniscus and a modified racking hitch knot tied in one goes closing the fish mouth.
Conclusion: This modification (HP knot) saves operative time, it is cost-effective and has the distinct advantage of a reduction in the size of the final knot construct.
Keywords: Horizontal cleavage tears, fish mouth closure, racking hitch knot.
Horizontal cleavage meniscus tears are a common orthopedic injury [1]. Horizontal cleavage tears (HCT) of the meniscus are treated with debridement of the flaps, rasping the edges, and closure of the flaps with sutures to achieve stable repair. Various methods are used to accomplish the repair, including an all-inside device [2, 3] or using a suture passing device [4, 5] and taking a bite through both flaps of the meniscus, using a sliding knot and half hitches. We used a modification of the racking hitch knot for repair of horizontal cleavage tear of the meniscus.
The patient is supine under spinal anesthesia with lateral thigh support applied at the level of the tourniquet. Standard arthroscopy portals are created for meniscus repair. Pie crusting of the medial collateral ligament is done to prevent the scuffing of the cartilage. The portals are switched to get a proper trajectory for the passage of the suture passing device. After debridement of the horizontal cleavage tear (Fig. 1a), a single bite is taken through both the flaps with a no. 0 fiber wire using the antegrade suture passing device (Fig. 1b). The fiber wire loop is then delivered through the working portal (Fig. 1c).
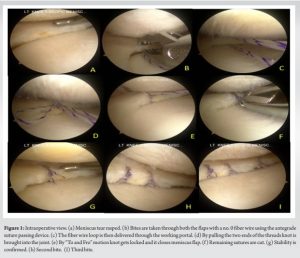
Then, the surgeon places the thumb and index finger down to up through the loop, and the same strands of thread are held to make a double loop (Fig. 2a, b, and c). The loop should look similar to what is shown in Fig. 2d. Both suture tails are passed through the double loop in opposite directions to each other (Fig. 2e, f, and g). The two ends of the suture are pulled, drawing a knot into the joint (Fig. 1d and Fig. 2h). This maneuver closes the meniscus flaps on each other (Fig. 1e and Fig. 2i). The knot is self-locking and gets tightly secured by making the suture tails rock in a “To and Fro” fashion. With the help of a suture cutter, the remaining threads are cut (Fig. 1f and Fig. 2j). This procedure is repeated multiple times as per the extent of tear (Fig. 1h and i).

Clinical reports on horizontal cleavage tear repair had shown good results [6, 7]. Kurzweil et al. in their systematic review reported a 78% healing rate [7]. Options available for fish mouth closure of horizontal cleavage tear of medial meniscus are either take one superior and one inferior capsular bite by inside out or all inside device such as fast fix or pass fiber wire through both the flap of the meniscus using suture passing device and tie the knot manually. Though it is time-saving, there is always a cost concern for using all inside devices. The inside-out technique needs the use of a safety incision, which adds to the operative time [8]. Passing fiber wire through the meniscus flap and manually tying the knot is cost-effective, but it needs multiple knots to secure it. Hence, it adds time to operative procedures, especially in tight joints. Furthermore, the final knot could be bulkier. Sanada et al. [9] used a raking hitch knot [10, 11] for all-inside repair for a radial tear at the posterior horn of the lateral meniscus. They recommended multiple half hitches to secure the knot, which adds to the time of the procedure. We tried modifying the racking hitch knot to take advantage of all the methods, i.e., cost-effectiveness and saving operative time. Our modified racking hitch knot (HP knot) is self-locking. The knot is complete in one step, it does not need a cannula as only a single bite is taken, saving operative time, especially in tight joints. We have confirmed the stability of the knot on the model as well as intraoperatively by pulling the knot with the probe. Furthermore, the knot is relatively less bulky, so concern about rubbing it against the femoral condyle is minimized. It is cost-effective as well.
Our modification of the racking hitch knot (HP knot) for fish mouth closure of horizontal cleavage tear of the meniscus is cost-effective and time-saving. The final knot is less bulky.
Modified racking hitch knot is a time-saving and cost-effective solution for closure of horizontal cleavage tear of the meniscus.
References
- 1.Metcalf MH, Barrett GR. Prospective evaluation of 1485 meniscal tear patterns in patients with stable knees. Am J Sports Med 2004;32:675-80. [Google Scholar]
- 2.Tiftikçi U, Serbest S. Repair of isolated horizontal meniscal tears with all-inside suture materials using the overlock method: outcome study with a minimum 2-year follow-up. J Orthop Surg Res 2016;11:131. [Google Scholar]
- 3.Woodmass JM, Johnson JD, Wu IT, Saris DB, Stuart MJ, Krych AJ. Horizontal cleavage meniscus tear treated with all-inside circumferential compression stitches. Arthrosc Tech 2017;6:e1329-33. [Google Scholar]
- 4.Brooks KR. Vertical lasso and horizontal lasso sutures for repair of horizontal cleavage and horizontal oblique meniscal tears: Surgical technique and indications. Arthrosc Tech 2017;6:e1767-73. [Google Scholar]
- 5.Accadbled F, Cassard X, Sales de Gauzy J, Cahuzac JP. Meniscal tears in children and adolescents: Results of operative treatment. J Pediatr Orthop B 2007;16:56-60. [Google Scholar]
- 6.Rubman MH, Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscal tears that extend into the avascular zone. A review of 198 single and complex tears. Am J Sports Med 1998;26:87-95. [Google Scholar]
- 7.Kurzweil PR, Lynch NM, Coleman S, Kearney B. Repair of horizontal meniscus tears: A systematic review. Arthroscopy 2014;30:1513-1. [Google Scholar]
- 8.Magnussen RA, Mather RC, Taylor DC. Arthroscopy-assisted inside-out and outside-in meniscus repair. In: Scooty IN, editor. Insall & Scott Surgery of the Knee. 5thed. Philadelphia, PA: Churchill Livingstone; 2012. p. 275-82. [Google Scholar]
- 9.Sanada T, Iwaso H, Honda E, Yoshitomi H, Inagawa M. All-inside repair for radial tear at the posterior horn of the lateral meniscus: A figure-8 suture technique. Arthrosc Tech 2021;10:e1973-7. [Google Scholar]
- 10.Eyberg BA, Walker JB, Harmsen SM, Gobezie R, Denard RJ, Lederman ES. Suture cerclage for stabilizing the humeral shaft during shoulder arthroplasty. JSES Int 2020;4:688-93. [Google Scholar]
- 11.Marissen R, Nelis M, Janssens M, Meeks M, Maessen J. A comparison between the mechanical behaviour of steel wires and ultra high molecular weight poly ethylene cables for sternum closure. Mater Sci Appl 2011;2:1367-74. [Google Scholar]