
Arthroscopic fixation of posterior cruciate ligament avulsion fracture using a single tibial tunnel and suture loop with Endo button is a simpler procedure with a good functional outcome.
Dr. H Varrdhaman Dhariwal, Department of Orthopaedics, Stanley Medical College, Chennai, Tamil Nadu, India. E-mail: varrdh@gmail.com
Introduction: A prospective case series study to analyze the outcome of arthroscopic fixation of posterior cruciate ligament (PCL) avulsion fracture using a single tibial tunnel and suture loop with button configuration technique. PCL avulsion fracture injury requires surgical treatment to restore PCL function and stability of the knee joint. Several open and arthroscopic procedures which require a steep learning curve are followed to treat these injuries; yet our technique is a simpler and safe technique with desirable outcomes and does not require a long learning curve. Hence, it is reported.
Case Series: Ten patients with the same ethnic background having avulsed PCL injury since 2015 underwent arthroscopic fixation of avulsed PCL with single tibial tunnel and suture loop with button configuration within 3 months of injury are studied prospectively till date. All patients are clinically and radiologically evaluated with varied parameters. Postoperatively structured rehabilitation protocol is followed for all the patients. Post-operative clinical and radiological assessments are done and analyzed in 6 weeks, 3 months, 6 months, 1 year, 2 years, and 3 years.
Discussion: Ten patients were available for follow-up for a period of 6 months–3 years. Outcome analysis at the end of 3 years for all patients showed definitive improvement in the function of the knee statistically and functionally.
Conclusion: For patients with PCL avulsion fracture, arthroscopic fixation of PCL with a single tibial tunnel and suture loop with Endo button configuration gives definitive results. Medium-term follow-up analysis shows no failure in the outcome.
Keywords: Tibial avulsed posterior cruciate ligament injury, arthroscopic fixation, single tibial tunnel, Endo button.
Posterior cruciate ligament (PCL) avulsion fracture is a type of avulsion fracture of the knee that represents the most common isolated PCL lesion. This involves the separation of the posterior tibial insertion of the PCL to variable degrees. Avulsion of PCL at its insertion is the most common PCL-isolated lesion accounting for 15% [1]. The mode of injuries is mostly related to RTA. In these injuries, posteriorisation forces occur against the tibia in a flexed knee posing maximum insult to PCL along its axis. PCL avulsion injuries are also seen in individuals who jump and land on a plantar flexed foot while the knee in flexed position. Fixation of avulsed fracture has provided better outcome [2] compared with the conservative management. Open surgical methods [3, 4] involving a posterior approach to the knee for reduce and fix the fracture pose serious injury to popliteal neurovascular structures and delayed recovery. To avoid damage to the same, arthroscopic methods [2, 5, 6] are safer, easier, and less invasive. Several methods [7] of arthroscopic fixation are being followed for the same. This study describes the fixation with a simpler single tibial tunnel technique and suture loop [8] with Endobutton configuration technique. This method is suitable for patients with large fragments, smaller fragments, and comminuted fragments with or without dislocations.
This is a prospective study conducted in our center since 2015. All skeletally matured patients <65 years of age with unilateral knee complaints and a history of injury to the knee were included in the study. Initial general and local clinical examinations were done. Thorough pre-operative evaluation for ruling out other systemic injuries was also done. Special tests for PCL laxity such as posterior drawer test, sag sign, and other knee examination tests were done. Routine radiographs (Fig. 1a and b) of both knees in standing anteroposterior and lateral views were taken. PCL stress view was also taken. Computed tomography scan of the affected knee to assess the avulsed fragment size and displacement was done. MRI knee was done to assess the ligament status. Patients with associated meniscus injury that may or may not require repair were also included in the study. Patients with PCL avulsion injury along with systemic illness who were not fit under anesthesia protocol were not included in the study. Informed consent for surgery and study was obtained beforehand for all the patients. Surgery was done within 3 months of injury. The Institutional Ethical Committee approval was obtained.

Operative technique
Under sterile aseptic precaution, the patient is in a supine position under regional anesthesia, through the standard anterolateral portal hematoma is washed out first. Diagnostic arthroscopy is performed, and other injuries were managed. A sloppy anterior cruciate ligament (ACL) sign with significant PCL laxity is observed. Through a high anteromedial portal intervening fat between ACL and PCL excised so as to create two posteromedial portals (high – viewing portal and low – working) (Fig. 2a) [9]. Care is taken to avoid iatrogenic injury to ACL and PCL fibers. Once the posteromedial compartment is visualized, a high posteromedial portal is created. Through the portal, a plane is created between the posterior aspect of PCL and the posterior joint capsule. Then a low posteromedial portal is created for passing the transparent 8 mm cannula. High posteromedial portals are utilized as visual portals while others as working portal. PCL and posterior capsule plane development was further progressed, and debridement of the avulsed fracture fragment is done. The base of the fracture crater has been debrided and freshened. Now PCL jig (Fig. 2b) is used to make a hole below the avulsed fracture fragment. Guide pin passed. The posterior cortex is pierced with a gentle tap. PCL protector guide kept in the guide pin and over-drilled with 4.5 mm cannulated drill bit. 5 Ethibond passed (Fig. 2c) from anteromedial and lateral to the PCL forming a loop around the PCL and then retrieved to the posteroinferior portal. Now, a knot around the PCL at the osteoligamentous junction using Samsung medical center knot is made. The Endobutton is threaded with the two limbs of the Ethibond and fixed at the base of the avulsed PCL fragment. Two threads from the posterior portal were passed and retrieved anteriorly through the tibial tunnel with a hook (Fig. 2d, e, and f) and a knot pusher technique. Fragment reduction is done and held in position with the help of Ethibond and Endobutton around the PCL. Alternatively, if the fragment is big, the tunnel will be taken through the fragment and if the fragment is small, the tunnel will be made a little inferior, and then the loop is taken around the avulsed fragment (Fig. 2g and h). After ensuring satisfactory reduction (Fig. 2i) and tension of the PCL, Ethibond fixed to the proximal tibia with Endobutton.

post-operative protocol
Isometric quadriceps strengthening exercises started on the 1st post-operative day. Non-weight bearing [10, 11] for 3 weeks post-operative period. Knee bending allowed to 0–90° for first 6 weeks. The first 6 weeks of closed chain exercise have been allowed, following which open chain exercises were followed, allowing the patient on full weight-bearing with quadriceps and hamstrings strengthening exercises.
A statistically significant difference in the mean pre-operative PCL stress radiograph score and mean post-operative PCL stress radiograph (Fig. 1e) score with P < 0.05 is noted. The statistically significant difference in mean between pre-operative and post-operative Tegner Lysholm scores and IKDC at 3 months, 6 months, 1 year, 2 years, and 3 years with P < 0.05 (Table 1) is noted.

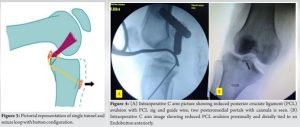
Statistically significant difference in mean between pre-operative and post-operative scores established stating this study acceptable. A variety of techniques have been done for displaced PCL avulsion such as the traditional Burks and Schaffer approach and posterior approach technique. The posterior approach for open reduction and internal fixation of PCL avulsion fractures was found to be effective in fractures involving large fragment. However, this method is highly invasive with a risk of neurovascular damage. When the fragment size is small and comminuted, it is difficult to fix through traditional technique. Various arthroscopic techniques such as arthroscopic suture tunnel pull-out technique are followed in most cases which enable accurate examination and visualization of the fragment and bone bed, as well as the ability to pull the fixation wire/thread from posterior to anterior side of the fragment. Our technique (Fig. 3) Single tunnel through the tibia with a loop around the PCL (Fig. 1c and d) has been advocated with the addition of Endobutton which helps in reduction of the fracture and even distribution of stress needed for fracture reduction of the avulsed PCL fragment. Arthroscopic fixation using a suspensory fixation device does not require a posterolateral portal. An excellent view of the transeptal region is obtained through the posteromedial portal. The present surgical technique is more convenient and less invasive and provides satisfactory fixation (Fig. 4) of the fracture fragments.
For patients with PCL avulsion fracture, our technique gives definitive results. Medium-term follow-up analysis shows no failure in the outcome (Fig. 1g, h, and i). Yet, medium- and long-term follow-up along with multi-centric trial is required.
The definitive purpose of this study is to highlight the successful management of PCL avulsion fracture injuries with arthroscopic technique. Among various available techniques of arthroscopic fixation with multiple tibial tunnels and multiple posterior ports, our technique uses only a single tibial tunnel and two posteromedial portals alone minimally disturbing the biology. Securing a loop around the avulsed fragment and augmenting its stability by adding an Endobutton ensures a satisfactory reduction of the avulsed fragment enabling faster recovery and providing an excellent outcome in medium-term follow-up.
References
- 1.Meyers MH. Isolated avulsion of the tibial attachment of the posterior cruciate ligament of the knee. J Bone Joint Surg 1975;57:669-72. [Google Scholar]
- 2.Sasaki SU, da Mota e Albuquerque RF, Amatuzzi MM, Pereira CA. Open screw fixation versus arthroscopic suture fixation of tibial posterior cruciate ligament avulsion injuries: A mechanical comparison. Arthroscopy 2007;23:1226-30. [Google Scholar]
- 3.Chen W, Luo W, Chen Z, Jiang Y. Treatment of posterior cruciate ligament avulsion fractures of the tibia using a toothed plate and hollow lag screw. Singapore Med J 2016;57:39-44. [Google Scholar]
- 4.Seitz H, Schlenz I, Pajenda G, Vécsei V. Tibial avulsion fracture of the posterior cruciate ligament: K-wire or screw fixation? A retrospective study of 26 patients. Arch Orthop Trauma Surg 1997;116:275-8. [Google Scholar]
- 5.Chen CH, Chen WJ, Shih CH. Fixation of small tibial avulsion fracture of the posterior cruciate ligament using the double bundles pull-through suture method Trauma 1999;46:1036-8. [Google Scholar]
- 6.Kim SJ, Shin SJ, Cho SK, Kim HK. Arthroscopic suture fixation for bony avulsion of the posterior cruciate ligament. Arthroscopy 2001;17:776-80. [Google Scholar]
- 7.Zhao J, He Y, Wang J. Arthroscopic treatment of acute tibial avulsion fracture of the posterior cruciate ligament with suture fixation technique through Y-shaped bone tunnels. Arthroscopy 2006;22:172-81. [Google Scholar]
- 8.Torisu T. Avulsion fracture of the tibial attachment of the posterior cruciate ligament. Indications and results of delayed repair. Clin Orthop Relat Res 1979;143:107-14. [Google Scholar]
- 9.Hooper PO 3rd, Silko C, Malcolm TL, Farrow LD. Management of posterior cruciate ligament tibial avulsion injuries: A systematic review. Am J Sports Med 2018;46:734-42. [Google Scholar]
- 10.Kan H, Nakagawa S, Hino M, Komaki S, Arai Y, Inoue H, et al. Arthroscopic fixation technique for avulsion fracture of the posterior cruciate ligament from the tibia. Arthrosc Tech 2020;9:e1819-24. [Google Scholar]
- 11.Ahn JH, Ha CW. Posterior trans-septal portal for arthroscopic surgery of the knee joint. Arthroscopy 2000;16:774-9. [Google Scholar]






