
Immediate reimplantation of the talus after thorough debridement will give favorable functional outcomes.
Dr. Akash Nagnath Mane, Department of Orthopedic surgery, Manipal Tata Medical College, Manipal Academy of Higher Education, Manipal-576104, Karnataka, India. E-mail: dr.akashmane54@gmail.com
Introduction: Traumatic open total extrusion of talus without soft-tissue attachment and not associated with surrounding fracture is a very rare injury which requires very high energy impact. In literature, optimal treatment protocols are yet to be established. A few options described in literature are talectomy and tibiocalcaneal arthrodesis or reimplantation of talus which may be immediate or after some interval.
Case Report: A 28-year-old female suffered road traffic accident and had total open extrusion of talus without soft-tissue attachment, and we managed it with thorough debridement of the wound, saline irrigation, and immediate reimplantation of the talus with stabilization by delta frame external fixator. Proper pre- and post-operative antibiotic coverage was given as per protocol. We did not face post-operative infection, wound complication, and until 12 months followed up, there are some signs of avascular necrosis of the talus but the good functional outcome.
Conclusion: With this case experience, we suggest that this is the valid treatment protocol for total extrusion of the talus, and it will provide a better hindfoot mechanism, heel height, and the patient can resume his/her daily routine activity as early as possible.
Keywords: Tibiocalcaneal arthrodesis, talar extrusion, avascular necrosis of talus.
Traumatic extrusion of the talus is an uncommon injury and occurs following high-energy trauma. It represents 0.06% of all talar injuries and 2% of talar dislocation [1]. Mechanism of injury normally described as extreme dorsiflexion or plantar flexion associated with subtalar supination or pronation [2]. Most commonly talar extrusion occurs after a road traffic accident so obviously contaminated with soil and there is no soft-tissue attachment so infection, avascular necrosis, arthritis, and poor functional outcome are the known complications after these injuries. There are various treatment plans described in the literature. Talectomy and primary tibiocalcaneal arthrodesis are a recommended plan to avoid post-operative complications but recently primary talar reimplantation with thorough debridement is a famous recommendation proposed by some authors. In this article, we present 28-year-old female who had a total extrusion of the talus with a 12 cm open wound following a road traffic accident, and we managed this case with thorough debridement, talar reimplantation, and stabilization with an external fixator.
A 28-year-old female presented to the emergency department with d h/o RTA and had approximately a 12 cm lacerated wound over the anterolateral aspect of the right ankle (Fig. 1).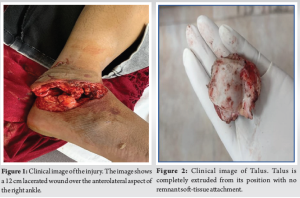 There is no other injury with stable vitals. The patient brought a piece of bone with her which was grossly contaminated (Fig. 2). As per open injury protocol, we thoroughly irrigated the wound in the emergency department and administered tetanus toxoid and triple antibiotics (Inj. Cefoperazone + Inj. Amikacin + Inj. Metronidazole). X-ray of the patient showed the absence of talus (Fig. 3). Hence, the diagnosis was made as “Total extrusion of talus without any fracture with a 12 cm open wound over anterolateral aspect of the ankle.” We planned an emergency surgery for thorough debridement and immediate reimplantation of the talus. In the operation theater, the patient was lying in a supine position under spinal anesthesia < thorough debridement of wound with 10 lit of normal saline was done, and all devitalized tissue debrided. Extruded talus soaked in betadine solution for 10 min and then reimplanted in its position.
There is no other injury with stable vitals. The patient brought a piece of bone with her which was grossly contaminated (Fig. 2). As per open injury protocol, we thoroughly irrigated the wound in the emergency department and administered tetanus toxoid and triple antibiotics (Inj. Cefoperazone + Inj. Amikacin + Inj. Metronidazole). X-ray of the patient showed the absence of talus (Fig. 3). Hence, the diagnosis was made as “Total extrusion of talus without any fracture with a 12 cm open wound over anterolateral aspect of the ankle.” We planned an emergency surgery for thorough debridement and immediate reimplantation of the talus. In the operation theater, the patient was lying in a supine position under spinal anesthesia < thorough debridement of wound with 10 lit of normal saline was done, and all devitalized tissue debrided. Extruded talus soaked in betadine solution for 10 min and then reimplanted in its position. 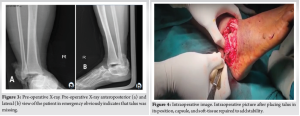 The ankle joint capsule and lateral collateral ligament were repaired (Fig. 4), after which the ankle appeared stable, which was confirmed under C-arm. Further stability was given by a delta frame external fixator (Fig. 5). Skin closure was done with low-tension sutures. Post-operative X-ray showed a well-reduced stable ankle with reimplanted talus (Fig. 6). Postoperatively, the limb was kept in strict elevation on the Bohler Braun frame, and after two dressings, the patient was discharged on post-operative day 5.
The ankle joint capsule and lateral collateral ligament were repaired (Fig. 4), after which the ankle appeared stable, which was confirmed under C-arm. Further stability was given by a delta frame external fixator (Fig. 5). Skin closure was done with low-tension sutures. Post-operative X-ray showed a well-reduced stable ankle with reimplanted talus (Fig. 6). Postoperatively, the limb was kept in strict elevation on the Bohler Braun frame, and after two dressings, the patient was discharged on post-operative day 5.  Sequential blood parameters assessed such as complete blood count, C-reactive protein which shows a downward trend and becomes normal within 2 weeks post-operative, and culture sensitivity done from wound swab which shows no bacterial growth. Suture removal was done after 20 days, and the patient was kept non-weight bearing for 12 weeks. The external fixator was removed after 12 weeks, and at that time, check X-ray did not show sclerosis or collapse of the talus (Fig. 7).
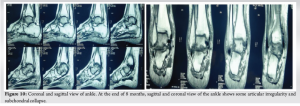
Sequential blood parameters assessed such as complete blood count, C-reactive protein which shows a downward trend and becomes normal within 2 weeks post-operative, and culture sensitivity done from wound swab which shows no bacterial growth. Suture removal was done after 20 days, and the patient was kept non-weight bearing for 12 weeks. The external fixator was removed after 12 weeks, and at that time, check X-ray did not show sclerosis or collapse of the talus (Fig. 7). Partial weight bearing was started (Fig. 8) with ankle range of motion (ROM) exercises. The patient did plantar flexion up to 30° and dorsiflexion up to 10° (Fig. 9). After 8 months, we planned a magnetic resonance imaging (MRI) of the right ankle which shows some articular irregularity (Fig. 10), but the patient started full weight bearing with a full ROM. We measured the functional outcome of the ankle with the American Orthopaedic Foot and Ankle Society scoring system at the end of 12 months which comes to 73. During the past follow–up, the patient started her routine daily work painlessly and comfortably (Fig. 11).
Partial weight bearing was started (Fig. 8) with ankle range of motion (ROM) exercises. The patient did plantar flexion up to 30° and dorsiflexion up to 10° (Fig. 9). After 8 months, we planned a magnetic resonance imaging (MRI) of the right ankle which shows some articular irregularity (Fig. 10), but the patient started full weight bearing with a full ROM. We measured the functional outcome of the ankle with the American Orthopaedic Foot and Ankle Society scoring system at the end of 12 months which comes to 73. During the past follow–up, the patient started her routine daily work painlessly and comfortably (Fig. 11).

Open total talar extrusion without attachment of any ligaments and without any fracture is a very rare injury and challenging to manage. Forceful plantar flexion and subtalar supination are the mechanism responsible for this injury. Normally, this extrusion is associated with malleolar fracture [3]. However, in our case, there was pure extrusion of talus without any associated fractures. Infection and avascular necrosis are the two most important complications associated with open talar extrusion. There is no muscular attachment to the talus and approximately 60% of the talus is covered with articular cartilage, this anatomical nature of the talus responsible for extrusion. With high-energy trauma, ligamentous structures ruptured and talar dislocation or extrusion occurred with open injury [4]. Talectomy followed by thorough debridement and talocalcaneal arthrodesis was a popular method of treatment for this injury earlier, but now, thorough debridement and reimplantation of talus give better functional outcomes than arthrodesis so it becomes 1st line of management [5]. Palomo-Traver et al. proposed that a totally extruded or grossly contaminated talus should be replaced [6]. Smith et al. [7] and Assal and Stern [8] reported in their respective study that a totally extruded talus should be managed with thorough debridement of the wound followed by reimplantation of the talus. Some authors, to reduce the risk of infection, postpone talus reimplantation, and use talus-shaped antibiotic cement while waiting for cultural results and then talus implantation done in a staged procedure [9]. Recent studies suggest that immediate reimplantation with thorough irrigation of wound and debridement of tissue leads to lesser chance of probable post-operative complications such as infection and avascular necrosis [9, 10]. We kept extruded talus for 10 min in diluted povidone-iodine solution to get rid of bacterial flora. After this implantation, we were also able to close the wound appropriately, so we did not encounter the need for secondary wound debridement or any skin grafting procedure. Some authors have reported in their study that reimplantation of an extruded talus with some soft-tissue attachments has relatively good clinical results [6]. However, in cases without any soft-tissue attachments, the result of reimplantation of a likely avascular and contaminated talus, which may act as a sequestrum, is questionable. In our case, there is no soft-tissue attachment as the talus is completely extruded and found roadside near the place of the accident though there is no sign of infection till 8-month follow-up, but some subchondral collapse was noted in MRI done at 8-month follow-up. After reimplantation, stabilization of the joint can be done with K wire fixation or Steinmann pins from the calcaneus through the talus into the distal tibia or using an external fixator [11-13]. In our case, we avoided any implant around the talus and stabilization was done with a delta frame external fixator which was a stable tibiotalar and subtalar joint. The patient is pain-free and started jogging, cycling, and jumping which indicates an extremely good functional outcome. Our only concern is long-term outcome, and avascular necrosis cannot be ruled out till 2-year post-injury.
Open total talar extrusion injury is challenging to manage for orthopedic surgeons. Our study with supportive recent literature suggests that early wound debridement, thorough antibiotic coverage, and immediate talar reimplantation are a favorable plan of management for preserving good ankle function, normal joint anatomy, and avoiding further reconstructive procedures.
Open total talar extrusion is a rare injury. There is a different way to manage this rare injury. Immediate implantation after thorough debridement and thorough antibiotic coverage is the preferred way of management to give good functional outcomes and also avoid post-operative wound-related complications.
References
- 1.Kwak JM, Heo SK, Jung GH. Six-year survival of reimplanted talus after isolated total talar extrusion: A case report. J Med Case Rep 2017;11:348. [Google Scholar]
- 2.Leitner B. The mechanism of total dislocation of the talus. J Bone Joint Surg Am 1955;37:89-95. [Google Scholar]
- 3.Montoli C, De Pietri M, Barbieri S, D’Angelo F. Total extrusion of the talus: A case report. J Foot Ankle Surg 2004;43:321-6. [Google Scholar]
- 4.Hiraizumi Y, Hara T, Takahashi M, Mayehiyo S. Open total dislocation of the talus with extrusion (missing talus): Report of two cases. Foot Ankle 1992;13:473-7. [Google Scholar]
- 5.Weston JT, Liu X, Wandtke ME, Liu J, Ebraheim NE. A systematic review of total dislocation of the talus. Orthop Surg 2015;7:97-101. [Google Scholar]
- 6.Palomo-Traver JM, Cruz-Renovell E, Granell-Beltran V, Monzonis-Garcia J. Open total talus dislocation: Case report and review of the literature. J Orthop Trauma 1997;11:45-9. [Google Scholar]
- 7.Smith CS, Nork SE, Sangeorzan BJ. The extruded talus: Results of reimplantation. J Bone Joint Surg Am 2006;88:2418-24. [Google Scholar]
- 8.Assal M, Stern R. Total extrusion of the talus. A case report. J Bone Joint Surg Am 2004;86:2726-31. [Google Scholar]
- 9.Issaoui H, Fekhaoui MR, Abbassi H, Gargouri M, Ali M. Outcomes of a reimplanted talus after a total open extrusion. Cureus 2020;12:e9678. [Google Scholar]
- 10.Mohindra M, Gogna P, Thora A, Tiwari A, Singla R, Mahindra P. Early reimplantation for open total talar extrusion. J Orthop Surg (Hong Kong) 2014;22:304-8. [Google Scholar]
- 11.Fleming J, Hurley KK. Total talar extrusion: A case report. J Foot Ankle Surg 2009;48:690.e19-23. [Google Scholar]
- 12.Van Opstal N, Vandeputte G. Traumatic talus extrusion: Case reports and literature review. Acta Orthop Belg 2009;75:699-704. [Google Scholar]
- 13.Karampinas PK, Kavroudakis E, Polyzois V, Vlamis J, Pneumaticos S. Open talar dislocations without associated fractures. Foot Ankle Surg 2014;20:100-4. [Google Scholar]







