
The combination of the two-stage approach with osteochondral allograft using a 3D planning contributed to preserve joint function and improve the quality life of this patient with a bipolar defect and history of infection.
Dr. Mauricio Zuluaga-Botero, Limb of Lengthening and Reconstruction Unit, Clínica Imbanaco Grupo QuirónSalud, Cali, Colombia. E-mail: info@mauriciozuluaga.com
Abstract
Introduction: Transplantation with fresh cadaveric osteochondral allograft (FOCA) is frequently used in defects of the femoral condyle and tibial plateau to preserve the knee joint. However, the use of FOCA in bipolar lesions remains controversial in cases with bipolar defects and a history of infection.
Case Report: We present a 21-year-old male patient with a massive post-traumatic osteochondral defect of the lateral compartment of the knee and a history of infection, treated by a two-stage approach. In stage 1, infection was eradicated, and joint function recovered with aggressive debridement, polymethyl methacrylate beads, bone cement spacers, and Judet’s quadricepsplasty. In stage 2, transplantation was performed with a bipolar FOCA. All treatments were planned using 3D-printed models.
Conclusion: The two-stage approach and 3D planning can increase the chances of transplant success by preparing the future allograft bed and obtaining an optimal match between the cadaveric allograft and the patient’s defect in cases with potential contraindications, such as a bipolar lesion in the femoral condyle and tibial plateau and a history of infection. A combined approach may lead to a more beneficial outcome for the patient to preserve joint function and improve quality of life.
Keywords: Osteochondral allograft, bone defect, 3D planning.
Transplantation with a fresh cadaveric osteochondral allograft (FOCA) is a treatment option in cases of osteochondral knee defects, mainly in young patients with high functional demand [1,2]. Compared to partial or total knee replacement, FOCA transplantation has evidenced better functional outcomes in the active population due to the lower risk of failure, allowing joint preservation in 70–90% of cases at a 10-year follow-up [3-5]. The use of FOCA in bipolar lesions is still a controversial issue because some reports have described poor results and a high risk of revision, so it has even been considered that bipolar defects are a contraindication for the procedure [1,3,6]. Another factor that could determine the success of the transplant is the history of infection because it can negatively impact the consolidation process, increase the risk of allograft infection, and consequently, decrease its survival [1,3]. This article describes a case report of a patient with a post-traumatic osteochondral defect of the lateral compartment of the knee with a history of infection who underwent secondary reconstruction using a two-stage approach with bipolar FOCA transplantation. Pre-surgical planning in both stages was optimized with 3D printing prototypes.
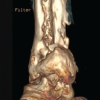
A 21-year-old male patient was involved in a traffic accident in April 2017, resulting in a Grade IIIB (Gustilo-Anderson Classification) exposed fracture of the left lower limb with soft tissue involvement and loss of the lateral compartment of the knee with a massive osteochondral defect. Initially, he was treated in another institution with a transarticular external fixator in extension, and the soft tissue defect was covered with a latissimus dorsi free flap and skin grafts in the leg. He developed graft necrosis, requiring multiple debridements. The defect was covered with an anterolateral right thigh-free flap and the edges with split-thickness skin grafts. At that moment, the patient refused a knee arthrodesis. Three months after the traumatic event, the patient was referred to our institution with moderate pain and purulent discharge from the proximal Schanz screws (Fig. 1). A two-stage surgical treatment approach was planned, including stage 1: eradication of infection and recovery of joint function and stage 2: transplantation with bipolar FOCA. Stage 1 started with the removal of the transarticular external fixator and debridement with femur and tibia sequestrectomy. Cultures were taken, and knee mobilization was performed; the defect was filled with polymethylmethacrylate beads (PMMA) mixed with gentamicin plus vancomycin. Oxacillin-sensitive Staphylococcus aureus was isolated, and intravenous cefazolin was indicated for 6 weeks. A computerized axial tomography (CAT) scan with 3D mirror reconstruction of both knees was requested for surgical planning to make the cutting guides and cats of the femoral condyle and the external tibial plateau (Fig. 2). The measurements of the defect in the tibia were anteroposterior 6 cm, transverse 8 cm, length 8 cm, and in the femoral condyle: anteroposterior: 7.3 cm, transverse 8.5 cm, and length 6 cm. Eight days after the first surgery, the second stage 1 procedure was performed to improve joint mobility. In this surgery, the reconstruction of the lateral compartment was performed with PMMA bone cement spacers, which were designed based on the 3D anatomical models (Fig. 2d). Functional recovery was achieved with a Judet’s quadricepsplasty, achieving a knee range of motion (ROM) of 0–90° (Fig. 3). Post-operatively, continuous passive mobilization machine therapy was initiated for 5 days, and physical therapy focused on improving ROM and pain with proprioception and quadriceps strengthening exercises; the patient also received education for walking with crutches. Cultures taken during this second surgery were negative, and cefazolin was continued until the treatment was completed. Once stage 1 was completed, the process of searching for a fresh allograft compatible in size with the patient’s tomographic measurements began. Due to delays in the approval of the FOCA transplantation by the health insurance company, stage 2 was initiated 15 months after the accident (or 12 months after the last surgery). At that time, radiographic follow-up showed preserved joint relationships and decreased femorotibial joint space with the osteosynthesis material in situ, with no sign of reactivation of the infection (Fig. 4). Once the allograft was obtained, X-rays and CAT scans of the allograft were taken to 3D-print the cutting guides and obtain an anatomical coupling between the defect and the fresh allograft. Before starting reconstructive surgery with FOCA, the 3D models were sterilized and sealed. Digital planning and cutting guides were performed according to the 3D reconstruction in Fig. 2. The cement spacers in the femur and tibia, as well as all the osteosynthesis material, were removed, and with the help of cutting guides, the defect was regularized to maximize the articular congruence of the femoral condyle and the external tibial plate. Bone tunnels were made in the femur, tibia, and fibula for anatomical ligament reconstruction. The allograft was fixed with interferential screws and plates in the distal femur and proximal tibia under fluoroscopic visualization. Reconstruction of the posterolateral corner, including the lateral collateral ligament, the popliteofibular ligament, and the popliteus tendon, was performed using the technique described by Chang et al., [7] achieving adequate joint stability. As shown in Fig. 5 and 3D printing, surgical guides allowed an anatomical and congruent joint reconstruction of the articular surface. Since the first post-operative day, the rehabilitation process has begun with isometric quadriceps exercises, active/active-assisted ROM exercises, and gait training with partial load. On the 5th post-operative day, the patient left the institution with adequate pain control and a ROM of 0–40°. Post-operative radiographs showed recovery of joint congruency, alignment, and adequate fixation of the bipolar FOCA (Fig. 6). During follow-up, no complications were reported, and there were no signs of infection reactivation. At the last follow-up, 5 years after transplantation with FOCA, the patient reported no functional limitations (mobility, self-care, usual activities) or pain but reported moderate symptoms of anxiety or depression through the EQ-5D-3L questionnaire. Nevertheless, he rated his overall health status with a score of 90 on a scale of 0–100. The final ROM of the left knee was 0–90°, without functional instability. Fig. 7 shows the radiological follow-up at the last control. The patient provided consent for publication.
Reconstruction of massive osteochondral defects of the lateral compartment of the knee in young, active patients is a challenge due to the need to provide a reconstruction that lasts over time while achieving a return to activities of daily living with the best possible functionality. FOCA transplantation is considered an innovative and cost-effective long-term treatment approach for the young population because it preserves most of the patient’s native biological structure while allowing a return to activities of daily living and post-poning the need for joint replacement [8]. In this study, a two-stage surgical treatment approach was described in a case with a massive osteochondral defect, which can be considered complex due to bipolar involvement and a history of infection. These last two conditions have been described as frequent causes of failure in the literature [1,3], so they may have a decisive impact on the success of transplantation. However, in this young 21-year-old patient, FOCA transplantation was preferred to joint replacement given the need for revision at an expected time of 10–15 years. Consequently, two-stage management was designed to provide a more comprehensive approach and minimize the risk of infection reactivation. In stage 1, eradication of the infection was achieved with an aggressive approach based on debridements and resection of scar tissue and bone surfaces, plus targeted antibiotic therapy. Due to the prolonged time without mobilization and the high risk of reinfection, a temporary reconstruction was performed to restore joint function by reconstructing the defect with a custom-fitted articulating PMMA spacer and Judet’s quadricepsplasty. This stage before transplantation with FOCA was key to guarantee an adequate recipient bed that would allow biological integration with the future allograft. In this patient, definitive reconstruction of the bone defect was performed in stage 2 with a 3D model-based FOCA transplantation. Additionally, due to the complexity of the defect, multidisciplinary management was performed with a specialist in the reconstruction of multiligamentary knee injuries. With this treatment approach, a favorable clinical and functional outcome was achieved at 5 years post-operatively, which could be attributed in part to the optimal coupling achieved with the use of 3D guides between the cadaveric allograft and the patient’s defect [9] since it has been described that the degree of fit can be decisive in determining the viability of the chondrocytes and allograft regeneration [10]. The advantages of using 3D planning in performing a FOCA transplant were also highlighted by Huotilainen et al., [11] who described their experience with a 40/28.5/24 mm unipolar defect (medial-lateral/superior-inferior/anterior-posterior), highlighting that the implementation of 3D models improves allograft fit and facilitates the surgical procedure. In our experience, another advantage of using 3D planning is to optimize the articular congruence of the femoral condyle, which can be more difficult due to the existing curved articular surface and variations in femoral size between subjects. Ensuring this congruence between donor and recipient improves the contact surface in the metaphyseal areas and benefits the osseointegration process.
The two-stage approach and 3D planning can increase the chances of transplant success by preparing the future allograft bed and obtaining an optimal coupling between the cadaveric allograft and the patient’s defect in cases with potential contraindications, such as a bipolar lesion in the femoral condyle and the tibial plateau and a history of infection. A combined approach can lead to a more beneficial outcome for the patient to preserve joint function and improve quality of life.
In young patients with potential contraindications, such as massive defects and infection, transplantation with FOCA is a good option provided that a comprehensive surgical approach is taken to reduce potential complications.
References
- 1.Cavendish PA, Everhart JS, Peters NJ, Sommerfeldt MF, Flanigan DC. Osteochondral allograft transplantation for knee cartilage and osteochondral defects: A review of indications, technique, rehabilitation, and outcomes. JBJS Rev 2019;7:e7. [Google Scholar | PubMed]
- 2.Hohmann E, Tetsworth K. Large osteochondral lesions of the femoral condyles: Treatment with fresh frozen and irradiated allograft using the Mega OATS technique. Knee 2016;23:436-41. [Google Scholar | PubMed]
- 3.Chui K, Jeys L, Snow M. Knee salvage procedures: The indications, techniques and outcomes of large osteochondral allografts. World J Orthop 2015;6:340-50. [Google Scholar | PubMed]
- 4.Schmidt KJ, Tírico LE, McCauley JC, Bugbee WD. Fresh osteochondral allograft transplantation: Is graft storage time associated with clinical outcomes and graft survivorship?. Am J Sports Med 2017;45:2260-6. [Google Scholar | PubMed]
- 5.Pisanu G, Cottino U, Rosso F, Blonna D, Marmotti AG, Bertolo C, et al. Large osteochondral allografts of the knee: Surgical technique and indications. Joints 2018;6:42-53. [Google Scholar | PubMed]
- 6.Kunze KN, Ramkumar PN, Manzi JE, Wright-Chisem J, Nwachukwu BU, Williams RJ 3rd. Risk factors for failure after osteochondral allograft transplantation of the knee: A systematic review and exploratory meta-analysis. Am J Sports Med 2023;51:1356-67. [Google Scholar | PubMed]
- 7.Chang CB, Seong SC, Lee S, Yoo JH, Park YK, Lee MC. Novel methods for diagnosis and treatment of posterolateral rotatory instability of the knee. J Bone Joint Surg Am 2007;89:2-14. [Google Scholar | PubMed]
- 8.Mistry H, Metcalfe A, Smith N, Loveman E, Colquitt J, Royle P, et al. The cost-effectiveness of osteochondral allograft transplantation in the knee. Knee Surg Sports Traumatol Arthrosc 2019;27:1739-53. [Google Scholar | PubMed]
- 9.Meng M, Wang J, Sun T, Zhang W, Zhang J, Shu L, et al. Clinical applications and prospects of 3D printing guide templates in orthopaedics. J Orthop Translat 2022;34:22-41. [Google Scholar | PubMed]
- 10.Sherman SL, Garrity J, Bauer K, Cook J, Stannard J, Bugbee W. Fresh osteochondral allograft transplantation for the knee: Current concepts. J Am Acade Orthop Surg 2014;22:121-33. [Google Scholar | PubMed]
- 11.Huotilainen E, Salmi M, Lindahl J. Three-dimensional printed surgical templates for fresh cadaveric osteochondral allograft surgery with dimension verification by multivariate computed tomography analysis. Knee 2019;26:923-32. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect with Titanium Cage Combined with the Masquelet Technique: A Case Report January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions
January 1, 2026 Harnessing 3D Printing Technology for Complex Acetabular Reconstruction in Revision Total Hip Arthroplasty: From Childhood Hip Trauma to Customized Modern Solutions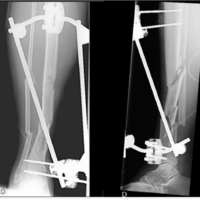 September 1, 2024 Masquelet Technique Combined with Ilizarov External Fixator, Reamer-irrigator-aspirator, and Flap Transplantation in an Open Tibial Fracture: A Case Report
September 1, 2024 Masquelet Technique Combined with Ilizarov External Fixator, Reamer-irrigator-aspirator, and Flap Transplantation in an Open Tibial Fracture: A Case Report June 29, 2021 Filling Bone Defects after Hip Arthroplasty Revision Using Hydroxyapatite/β-tricalcium Phosphate: A Case Report with Long-term Result
June 29, 2021 Filling Bone Defects after Hip Arthroplasty Revision Using Hydroxyapatite/β-tricalcium Phosphate: A Case Report with Long-term Result