
Suspicion of the possibility of alkaptonuria in a patient with atypical fracture presentation is important.
Dr. Arun John Paul, Department of Orthopaedics, Mission India Hospital, Khadgaon, Nagpur, Maharashtra, India. E-mail: arunjohnpaul87@gmail.com
Introduction: Alkaptonuria is a rare autosomal recessive genetic disorder found in 2–5/million live births. It results in dark brown pigmentation of connective tissues including cartilage and joint capsule that can often lead to arthropathy of large joints. However, bone fractures are unusual. This article describes a fracture neck of the femur in a patient with undiagnosed alkaptonuria managed at a rural center.
Case Report: A 60-year-old daily wage laborer with previously pain-free hips presented with sudden onset pain in the left hip while walking with no prior history of trauma. Radiographs showed a displaced fracture of the neck of the left femur. She underwent Left hip hemiarthroplasty. Intraoperatively, her soft-tissue including the joint capsule and the femoral head had dark brown pigmentation. Postoperatively, her urine was tested and the same turned black supporting the clinical diagnosis of alkaptonuria. At her 1-year follow-up, she had a painless, stable, and mobile hip.
Conclusion: We report a rare and unique case of neck of femur fracture in a patient with alkaptonuria treated with hemiarthroplasty in a resource-limited hospital in rural India. It is essential to consider the possibility of this condition when we come across a patient with an atypical fracture presentation. This article also presents an overview of alkaptonuria with a discussion on etiopathogenesis, clinical presentation, diagnosis, and management.
Keywords: Hemiarthroplasty, ochronosis, black pigment, homogentisic acid.
Alkaptonuria is a rare autosomal recessive genetic disorder. It is present in 2–5 per million live births [1]. It is among the first genetic disorders described in humans that followed the Mendelian recessive inheritance principles. It was historically used by Archibald Garrod to illustrate “inborn errors of metabolism” principles in his Croonian lectures. The first case of alkaptonuria dates back as far as 1500 BC in the Egyptian mummy Harwa. This disease was discovered in 1866 by Virchow, who noticed the homogentisic acid pigment which was pale brownish yellow color (ochre-like) under microscopy [2]. Alkaptonuria results in dark brown pigmentation of connective tissues including cartilage and joint capsule that can often lead to arthropathy of large joints [3]. The organ systems usually affected are musculoskeletal, genitourinary, cardiovascular, eye, and skin [4]. Even though it causes osteopenia and osteoporosis of the bones, fractures are unusual which is evident from the limited literature available. This article describes a fractured neck of the femur in a 60-year-old lady with undiagnosed alkaptonuria managed at a rural resource-limited center in central India. We have also reviewed the etiopathogenesis, clinical features, and management of alkaptonuria from the available literature.
A 60-year-old lady who was socially active and worked as a daily wage laborer on an agricultural farm presented with an acute onset of pain in her left hip and an inability to weight bear. There was no history of recent trauma or fever. She did not have complaints of hip pain before this episode. She did not have any known medical illnesses although she was taking over-the-counter medications for breathlessness. She chewed tobacco for over 20 years and consumed alcohol for over 10 years. She was independent in her activities of personal care and hygiene. On examination, she was conscious, alert, and oriented to time, place, and person. Her vital signs were stable. Her left lower limb was shortened and externally rotated. She had left hip anterior joint line tenderness. Left hip range of movements was painfully restricted. She did not have any distal neurovascular deficits. A plain radiograph of the left hip showed a displaced fracture of the neck of the left femur (Fig. 1). She was offered left total hip arthroplasty due to her age and activity level to which she refused due to financial constraints. Therefore, she was planned for a left hip hemiarthroplasty; the same was performed through a modified Hardinge approach to the hip in the lateral position under spinal anesthesia. Intraoperatively, her soft-tissues including the joint capsule were thickened and had dark brown pigmentation. After exposure of the hip joint, the femoral head was extracted and the acetabulum was inspected. It was found that the femoral head and the acetabular cartilage had dark brown pigmentation; however, there were no defects in the cartilage cap (Fig. 2). Left hip hemiarthroplasty was completed as planned. The left hip was stable post-reduction.

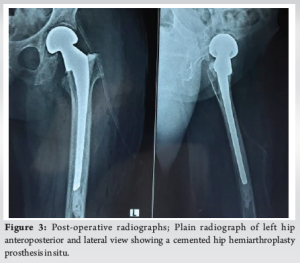
In the post-operative period, a clinical diagnosis of alkaptonuria was made and the same was further tested with her urine, which turned black on exposure to air. We screened her immediate family members after informed consent with the same urine test which revealed a positive test in two of them as well. The confirmatory urine homogentisic acid (HGA) test could not be performed due to the lack of access to the same. Her post-operative period was uneventful. The post-operative radiograph showed a satisfactory implant position (Fig. 3). She was started on full weight-bearing ambulation on the third post-operative day. She had a painless, stable, and mobile hip on further follow-up in the outpatient department. Her latest follow-up was 13-month post-surgery. She was not on any medications for pain. She was able to stand without support but required a cane to walk longer distances due to pain (Fig. 4). She was independent in her activities of personal care and hygiene. Due to the difficulty in walking, she was not employed since the surgery and was not active socially. She lived with her son’s family and was dependent on them financially.

There are a good number of publications on alkaptonuria presenting with arthritis but there are only a handful of case reports in the context of fractures. Ranganath et al. [5] described two cases of advanced alkaptonuria with coexisting osteoporosis. One patient developed multiple non-vertebral fragility fractures and the other patient developed vertebral fragility fractures while on nitisinone therapy and bisphosphonates therapy. Both were managed non-operatively with teriparatide injections for 2 years. Zacharia et al. [6] reported a patient with alkaptonuric ochronosis and scoliosis who suffered a fractured neck of the femur. This patient was planned for hip arthroplasty, but due to operative difficulties underwent hip excision arthroplasty. She was followed up for 3 years and was ambulant with a painless limp. Fisher et al. [7] reported a 69-year-old woman with alkaptonuria presenting with a low-energy trauma and distal femur fracture despite 2 years of alendronate therapy. She also had a history of severe arthritis requiring joint replacement surgeries in her right hip and both knees and aortic valve replacement surgery for severe aortic stenosis. She underwent retrograde femoral nailing following which she recovered well. Collins et al. [8] reported a 63-year-old man with alkaptonuric ochronosis who sustained a stress fracture of the neck of the left femur which necessitated surgical repair and recovered without any complications. Similarly, a stress fracture of the right femoral neck in a 73-year-old woman with alkaptonuria was reported by Park et al. [9] She recovered well after a total hip arthroplasty, and the right hip was pain-free at the 1-year follow-up. Alkaptonuria results from the deficiency of the enzyme Homogentisic acid 1,2 dioxygenase (HGD). This enzyme is found in the kidney, liver, colon, small intestine, and prostate [10] and plays an important role in tyrosine metabolism. In its absence, homogentisic acid (HGA) is produced in excess by the liver, which in turn is oxidized into an ochronotic pigment polymer that accumulates in the tissue causing ochronosis. The triad of alkaptonuria includes homogentisic aciduria, ochronosis, and ochronotic osteoarthropathy. The clinical features of alkaptonuria are secondary to ochronosis [7, 11-15]. It causes grey pigmentation of the sclera, ear cartilage, and skin. The respiratory reserve is decreased leading to restrictive lung disease. It affects the cardiovascular system causing arrhythmias and, an increase in the risk of coronary artery disease and valvular heart diseases including aortic stenosis and aortic regurgitation. It causes peripheral neuropathy, diplopia, and cerebrovascular accident. There is an increased incidence of gall bladder, renal, and prostatic stones. Our patient was neither diagnosed nor evaluated for alkaptonuria. Her history of intake of medications for breathlessness could be suggestive of restrictive lung disease or heart disease secondary to alkaptonuria. The patients in the other case reports had advanced ochronosis with systemic symptoms of the complications of alkaptonuria. The pathogenesis of alkaptonuria leading to osteoarthropathy is still unclear. It is found to be associated with loss of elasticity and increased hardness of hyaline cartilage [16]. The ochronotic pigment gets impregnated into the cartilage causing it to break down into fragments, especially in weight-bearing areas like the hip [17]. The bone changes in alkaptonuria are less severe than the cartilage changes. Even though the bone changes induced are similar to the changes in other connective tissues, the severity of the former appears to be limited because of calcification and bone remodeling. Furthermore, the bone collagen fibrils prevent the detrimental effects of the ochronotic pigment as they are encrusted by minerals and also because the new osteoid matrix remains uncalcified for too short to be modified by the ochronotic pigment [18]. Aliberti et al. [19] reported an increase in biochemical markers of bone resorption (increased urinary crosslinked N-telopeptides of collagen Type I) and an almost normal bone formation. This was seen in six out of the seven ochronotic patients indicating accelerated bone loss resulting in reduced bone mineral density. Ochronotic osteoarthropathy could cause premature arthropathy of the large and weight-bearing joints mainly in the spine, hips, knees, and shoulders. It affects the spine as early as the third decade and other joints often several years later; these could require joint replacement surgeries [7, 20]. The intervertebral discs in ochronotic spondyloarthropathy have extensive calcification which is characteristic and also shows a vacuum phenomenon. This is different from degenerative intervertebral discs and more closely resembles cartilage brittleness and fragmentation that occur in peripheral joints. Involvement of small joints of hands and feet typically seen in rheumatoid arthritis and features such as the bamboo spine, annular calcification, erosion, and sacroiliac fusion typically seen in ankylosing spondylitis do not occur in ochronotic spondyloarthropathy. At present, there is no cure for alkaptonuria. Treatment is mainly symptomatic and palliative like pain control, physiotherapy, and joint replacement surgeries. Vitamin C therapy is usually prescribed due to its ability to decrease the oxidation of HGA. However, there is no decrease in the urinary excretion of HGA even with Vitamin C therapy [11]. A low-protein diet can reduce the severity of the disease by reducing the tyrosine load. Nitisinone, a triketone herbicide has been shown to have a significant impact on alkaptonuria treatment. It inhibits the conversion of tyrosine to HGA. It results in reduced HGA levels in plasma and urine. But it causes increased levels of tyrosine in the body. This can lead to leukopenia, thrombocytopenia, porphyria, and corneal irritation [10, 11, 21]. The life expectancy of patients with alkaptonuria is usually normal; however, they have a significant decrease in the quality of life from as early as the fourth decade onwards, with symptoms such as lack of sleep, pain, and difficulty in breathing [10]. Hence, patient education and awareness are very crucial in this disease.
We report a rare case of fractured neck of the femur in an undiagnosed alkaptonuria patient treated with hip hemiarthroplasty at a resource-limited rural hospital in India. Active follow-up at their home, screening of family members, education, and management of the manifestations of this disease is essential to treat such patients from remote villages who would otherwise not seek any medical care.
Even though it is a rare disorder, suspicion and recognition of alkaptonuria preoperatively and intraoperatively are important in a patient presenting with hip fracture following trivial or no history of trauma.
References
- 1.Phornphutkul C, Introne WJ, Perry MB, Bernardini I, Murphey MD, Fitzpatrick DL, et al. Natural history of alkaptonuria. N Engl J Med 2002;347:2111-21. [Google Scholar]
- 2.Garrod AE. The incidence of alkaptonuria: A study in chemical individuality. Mol Med 1996;2:274-82. [Google Scholar]
- 3.Hamdi N, Cooke TD, Hassan B. Ochronotic arthropathy: Case report and review of the literature. Int Orthop 1999;23:122-5. [Google Scholar]
- 4.Gaines JJ Jr. The pathology of alkaptonuric ochronosis. Hum Pathol 1989;20:40-6. Erratum in: Hum Pathol 1989;20:500. [Google Scholar]
- 5.Ranganath LR, Khedr M, Mistry A, Vinjamuri S, Gallagher JA. Treatment of osteoporotic fractures in alkaptonuria by teriparatide stimulates bone formation and decreases fracture rate-a report of two cases. Bone Rep 2021;15:101151. [Google Scholar]
- 6.Zacharia B, Chundarathil J, Ramakrishnan V, Krishnankutty RM, Veluthedath R, Puthezhath K, et al. Black hip, fracture neck of femur and scoliosis: A case of ochronosis. J Inherit Metab Dis 2009;32:215-20. [Google Scholar]
- 7.Fisher AA, Davis MW. Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fracture: A case report and literature review. Clin Med Res 2004;2:209-15. [Google Scholar]
- 8.Collins EJ, Hand R. Alkaptonuric ochronosis: A case report. AANA J 2005;73:41-6. [Google Scholar]
- 9.Park BK, Egol KA. Displaced insufficiency femoral neck stress fracture in the setting of ochronosis: A case report. JBJS Case Connect 2014;4:e21. [Google Scholar]
- 10.Ranganath LR, Jarvis JC, Gallagher JA. Recent advances in management of alkaptonuria (invited review; best practice article). J Clin Pathol 2013;66:367-73. [Google Scholar]
- 11.Mistry JB, Bukhari M, Taylor AM. Alkaptonuria. Rare Dis 2013;1:e27475. [Google Scholar]
- 12.Gottschalk BH, Blankenstein J, Guo L. Ochronosis of mitral valve and coronary arteries. Ann Thorac Surg 2018;106:e19-20. [Google Scholar]
- 13.Olive JK, Alnajar A, Gnanashanmugam S, Lamelas J. Transcatheter aortic valve replacement for alkaptonuria-associated aortic stenosis. Ann Thorac Surg 2019;108:e377-9. [Google Scholar]
- 14.Keller JM, Macaulay W, Nercessian OA, Jaffe IA. New developments in ochronosis: Review of the literature. Rheumatol Int 2005;25:81-5. [Google Scholar]
- 15.Taylor AM, Wilson PJ, Ingrams DR, Helliwell TR, Gallagher JA, Ranganath LR. Calculi and intracellular ochronosis in the submandibular tissues from a patient with alkaptonuria. J Clin Pathol 2010;63:186-8. [Google Scholar]
- 16.Eberle P, Mohr W, Claes L. Biomechanical studies on the pathogenesis of ochronotic arthropathy. Z Rheumatol 1984;43:249-52. [Google Scholar]
- 17.Lagier R, Steiger U. Hip arthropathy in ochronosis: Anatomical and radiological study. Skeletal Radiol 1980;5:91-8. [Google Scholar]
- 18.Di Franco M, Coari G, Bonucci E. A morphological study of bone and articular cartilage in ochronosis. Virchows Arch 2000;436:74-81. [Google Scholar]
- 19.Aliberti G, Pulignano I, Schiappoli A, Minisola S, Romagnoli E, Proietta M. Bone metabolism in ochronotic patients. J Intern Med 2003;254:296-300. [Google Scholar]
- 20.Spencer JM, Gibbons CL, Sharp RJ, Carr AJ, Athanasou NA. Arthroplasty for ochronotic arthritis: No failure of 11 replacements in 3 patients followed 6-12 years. Acta Orthop Scand 2004;75:355-8. [Google Scholar]
- 21.Davison AS, Norman BP, Ross GA, Hughes AT, Khedr M, Milan AM, et al. Evaluation of the serum metabolome of patients with alkaptonuria before and after two years of treatment with nitisinone using LC-QTOF-MS. JIMD Rep 2019;48:67-74. [Google Scholar]





