
Timely recognition and meticulous arthroscopic management of pan-labral tears subsequent to a first-time shoulder dislocation are crucial for preventing future instability and premature osteoarthritis, highlighting the necessity for accurate diagnosis and precise surgical intervention.
Dr. Priyesh Kumar, Department of Orthopedics, Paras HMRI hospital, Patna, Bihar, India. E-mail: drpkojha27@gmail.com
Introduction: Pan-labral tears, commonly associated with recurrent shoulder dislocations, are a well-documented pathology. However, circumferential pan-labral tears following a first-time shoulder dislocation represent a rare and scarcely reported entity in the literature. Accurate diagnosis requires a comprehensive clinical history, physical examination, and further evaluation, often involving MRI. Even with advanced imaging, the acute nature of the injury can lead to the oversight of pan-labral tears, necessitating arthroscopic assessment for definitive diagnosis. Repairing such extensive glenoid labral tears presents a challenging task, requiring skilled surgeons to utilize accessory portals and percutaneous techniques for optimal visualization and anchor placement trajectory. To the best of our knowledge, this case report represents the first documentation of a pan-labral tear associated with a 1st-time shoulder dislocation.
Case Report: A 27-year-old Asian male presented with pain and limited range of motion in the left shoulder following a single episode of anterior shoulder dislocation during cricket. Initial X-rays were unremarkable, but subsequent MRI revealed an anteroinferior labral tear with intact rotator cuffs. Arthroscopic evaluation disclosed a pan-labral tear, prompting meticulous repair under general and locoregional anesthesia. The patient achieved full recovery postoperatively.
Conclusion: While pan-labral tears are typically linked to recurrent dislocations, this case underscores their occurrence in a 1st-time traumatic shoulder dislocation without overt clinical signs or fractures. Arthroscopic repair demands careful intraoperative planning to achieve optimal tensioning and alignment of labral and capsular tissues. This report contributes to the limited literature on pan-labral tears associated with initial shoulder dislocations, emphasizing the importance of arthroscopic evaluation for accurate diagnosis and successful repair.
Keywords: Shoulder dislocation, pan-labral tear, arthroscopy.
Glenoid labral tears in the shoulder, categorized as superior labral tears (SLAP lesions), anterior labral tears (Bankart lesions), and posterior labral tears (reverse Bankart lesions), represent common injuries with well-established classifications [1]. Notably, the superior and anteroinferior labrum are frequent anatomical sites for tears, with SLAP lesions described by Andrews et al. As posterosuperior labral tears extending anteriorly [2, 3]. Snyder et al., further, classified SLAP lesions into four categories, with SLAP type II being the most prevalent [4]. While combined tears of the anterior and superior labrum, as well as combined Bankart and SLAP tears, have been reported earlier [5, 6], recent descriptions include various combinations of labral lesions[7-9]. Powell et al. expanded the SLAP lesion classification with the introduction of type VIII and type IX, the latter being a circumferential or pan-labral tear involving multiple aspects of the labrum [9]. Circumferential glenoid labral tears, a rare entity in labral injuries, are often associated with traumatic events leading to instability and pain. Although it is hypothesized that these tears may initially be non-circumferential and evolve with subsequent instability events [10], it is noteworthy that a pan-labral tear can also occur with a single episode of dislocation. Due to potential limitations in imaging accuracy, diagnosis relies heavily on a thorough history, clinical examination, and heightened suspicion [7]. Arthroscopic repair of circumferential 360° labral tears has demonstrated success in restoring stability and reducing shoulder pain, allowing patients to return to pre-injury activity levels [10]. Surgeons should be prepared for intraoperative findings that may reveal a more extensive labral lesion than initially seen on imaging modalities. In this case report, we present the unique case of an athlete with a history of left shoulder trauma, demonstrating a pan-labral tear of the glenoid, who subsequently underwent successful arthroscopic repair. To the best of our knowledge, this represents the first documented case of its kind, highlighting the rarity and clinical importance of circumferential glenoid labral tears.
A 27-year-old right-hand dominant male presented with a single episode of anterior shoulder dislocation sustained during a cricket game. Following the incident, he reported persistent pain and limited range of motion in the left shoulder. Denying any neurological deficits, prior dislocations, shoulder injuries, or familial musculoskeletal disorders, the patient underwent a comprehensive clinical examination. Physical assessment revealed no deformity or muscle atrophy. Pain was noted during active and passive range of motion, particularly in abduction and flexion (Fig. 1). Laxity tests produced negative results, except for positive findings on the O’Brien and Apprehension tests. Neurological examination indicated preserved upper extremity strength and sensation.
Initial X-rays showed no abnormalities (Fig. 2), but subsequent MRI revealed an anteroinferior labral tear (Fig. 3). No rotator cuff abnormality was detected. Arthroscopy was planned to assess and address the confirmed 360° labral tear. Under general and loco-regional anesthesia, the patient underwent arthroscopy. A systematic examination explored various shoulder structures, confirming the extensive labral tear. The procedure began with addressing the superior-anterior labrum and biceps anchor tear. An accessory anterior-superior lateral portal was established with precision to avoid supraspinatus tendon violation. Using an outside-in spinal needle technique, the supraglenoid tubercle was freshened with a barrel burr.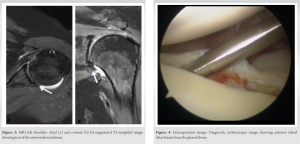
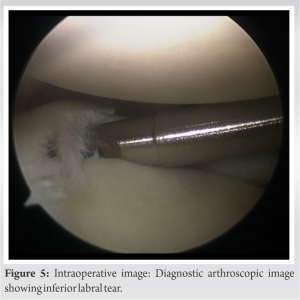
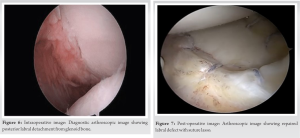
Arthroscopic inspection revealed the comprehensive nature of the labral tear, involving anterior, posterior, superior, and inferior aspects (Fig. 4-6). A meticulous repair processes followed, involving the use of portals and percutaneous techniques. Anchors were strategically placed to reattach the labrum and biceps anchor complex, ensuring proper tensioning and alignment (Fig. 7). The procedure concluded with subacromial bursectomy, closure, and placement of a shoulder immobilizer.
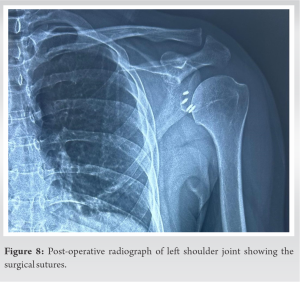
Postoperatively, the patient had an uneventful hospital stay and was discharged on the 2nd day after a post-operative check radiograph (Fig. 8). The case underscores the importance of clinical examination, advanced imaging, and arthroscopic confirmation in diagnosing and treating circumferential glenoid labral tears, even in the absence of recurrent dislocations.
Combined lesions of the glenoid labrum, involving multiple quadrants, are recognized as a unique glenohumeral pathological entity [1, 11]. The circle concept of instability proposes a biomechanical mechanism leading to circumferential glenoid labral tears. According to this concept, shoulder instability in one direction should be accompanied by a lesion on the opposite site; for instance, anterior shoulder instability should coincide with a posterior lesion [12, 13]. Although circumferential tears are commonly associated with multiple shoulder dislocations, they can also occur after a single traumatic event, challenging the notion that recurrent dislocations are a prerequisite [14]. MRI, despite being a widely used imaging modality, exhibits poor sensitivity in preoperatively identifying circumferential labral tears [15]. Surgeons should anticipate more extensive intraoperative findings, emphasizing the importance of obtaining preoperative information through medical history, physical examination, and imaging. It is crucial not to neglect even a single episode of shoulder injury and dislocation with a painful range of motion, especially if radiographs appear normal, as it may indicate a pan-labral lesion [16]. Left untreated, such lesions can lead to future instability and subsequent painful osteoarthritis [17].
Circumferential glenoid labral tears, typically associated with recurrent dislocations, can also occur after a single traumatic shoulder dislocation. Recent research challenges the assumed relationship between dislocation frequency and tear extent. Comprehensive evaluation, including arthroscopic inspection, is crucial as pan-labral tears may be missed in MRI studies. Arthroscopic repair yields favorable outcomes.
It is crucial to consider pan-labral tears even in cases of a first-time shoulder dislocation to avoid overlooking extensive injuries that may lead future instability and osteoarthritis, emphasizing the need for a comprehensive diagnostic approach and early arthroscopic intervention for favorable treatment outcomes.
References
- 1.Lo IK, Burkhart SS. Triple labral lesions: Pathology and surgical repair technique-report of seven cases. Arthroscopy 2005;21:186-93. [Google Scholar]
- 2.Zhu M, Chen JY, Chong HC, Cheng PC, Tjoen DL. Comparative study on clinical results of arthroscopic repair of anteroinferior, superior, and combined glenoid labral tear. J Orthop Surg 2018;26:2309499018762619. [Google Scholar]
- 3.Andrews JR, Carson WG Jr., Mcleod WD. Glenoid labrum tears related to the long head of the biceps. Am J Sports Med 1985;13:337-41. [Google Scholar]
- 4.Snyder SJ, Karzel RP, Del Pizzo WR, Ferkel D, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy 1990;6:274-9. [Google Scholar]
- 5.Gartsman GM, Roddey TS, Hammerman SM. Arthroscopic treatment of anterior-inferior glenohumeral instability. Two to five-year follow-up. J Bone Joint Surg Am 2000;82:991-1003. [Google Scholar]
- 6.Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med 1995;23:93-8. [Google Scholar]
- 7.Lindauer KR, Major NM, Rougier-Chapman DP, Helms CA. MR imaging appearance of 180-360 degrees labral tears of the shoulder. Skeletal Radiol 2005;34:74-9. [Google Scholar]
- 8.Mazzocca AD, Cote MP, Solovyova O, Rizvi SH, Mostofi A, Arciero RA. Traumatic shoulder instability involving anterior, inferior, and posterior labral injury: A prospective clinical evaluation of arthroscopic repair of 270° labral tears. Am J Sports Med 2011;39:1687-96. [Google Scholar]
- 9.Powell SE, Nord KD, Ryu RK. The diagnosis, classification, and treatment of SLAP lesions. Oper Tech Sports Med 2012;20:46-56. [Google Scholar]
- 10.Tokish JM, Mcbratney CM, Solomon DJ, Leclere L, Dewing CB, Provencher MT. Arthroscopic repair of circumferential lesions of the glenoid labrum. J Bone Joint Surg Am 2009;91:2795-802. [Google Scholar]
- 11.Owens BD, Nelson BJ, De Berardino TM. Arthroscopic repair of combined labral lesions. Tech Shoulder Elbow Surg 2008;9:10-4. [Google Scholar]
- 12.Dickens JF, Kilcoyne KG, Giuliani J, Owens BD. Circumferential labral tears resulting from a single anterior glenohumeral instability event: A report of 3 cases in young athletes. Am J Sports Med 2012;40:213-7. [Google Scholar]
- 13.Bäcker HC, Galle SE, Maniglio M, Rosenwasser MP. Biomechanics of posterior shoulder instability - Current knowledge and literature review. World J Orthop 2018;9:245-54. [Google Scholar]
- 14.Hasebroock AW, Brinkman J, Foster L, Bowens JP. Management of primary anterior shoulder dislocations: A narrative review. Sports Med Open 2019;5:31. [Google Scholar]
- 15.Maalouly J, Aouad D, Tawk A, Dib N, El Rassi G. Pan-labral tear of the shoulder joint in a non-athlete patient with six years history of recurrent shoulder subluxations and intraoperative findings of osteoarthritic changes: A case report. Trauma Case Rep 2020;26:100286. [Google Scholar]
- 16.Amorim E, Maganinho P, Rodrigues-Gomes D, Rodrigues-Gomes S, Sevivas N. Type IX superior labrum anterior and posterior lesion in a professional football player: A rare pattern of shoulder instability in a non-throwing athlete. Cureus 2023;15:e34753. [Google Scholar]
- 17.Aman ZS, Peebles LA, Johnson DW, Hanson JA, Provencher MT. Multidirectional shoulder instability with circumferential labral tear and bony reverse hill sachs: Treatment with 270° labral repair and fresh talus osteochondral allograft to the humeral head. Arthrosc Tech 2021;10:e781-7. [Google Scholar]








