
This case highlights the intricate challenges and complications that can arise from high-impact musculoskeletal trauma. The necessity for a multidisciplinary approach, involving orthopedic surgeons, radiologists, and physiotherapists, is evident in managing the diverse injuries and complications encountered. The importance of vigilant post-operative monitoring, especially in the context of persistent symptoms, is underscored, as it may unveil unforeseen issues such as ligamentous injuries and avascular necrosis.
Dr. Adnan Anwer, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.adnan.amu@gmail.com
Introduction: Central hip dislocations are rare orthopedic injuries, and their concomitant occurrence with ipsilateral knee dislocations is an even rarer phenomenon. We present a unique case of central hip dislocation along with ipsilateral knee dislocation and additional fractures involving the lateral condyle of the left tibia and patella. This complex injury pattern resulted from a severe road traffic accident, necessitating operative management to address the multiple musculoskeletal injuries. Ultimately, femoral head avascular necrosis (AVN) developed, leading to the need for total hip replacement (THR).
Case Report: A 28-year-old male was involved in a high-impact road traffic accident, leading to central hip dislocation, ipsilateral knee dislocation, and fractures of the lateral condyle of the left tibia and patella. The patient was promptly assessed, and operative intervention was initiated. Closed reduction and internal fixation with K-wires were performed for the fractures of the lateral condyle of the left tibia and patella. For the central hip dislocation, open reduction was achieved using a 9-hole RECON plate. Following the procedures, a long leg slab was applied for 6 weeks to facilitate optimal healing. Postoperatively, at the 6-week mark, K-wires were removed, and the patient commenced physiotherapy with partial weight-bearing permitted. However, during the rehabilitation phase, the patient reported instability in his left knee. Magnetic resonance imaging revealed an avulsion fracture of the posterior cruciate ligament (PCL) from its tibial attachment site and a complete anterior cruciate ligament (ACL) tear. It was observed that the femoral head had developed AVN. This complication necessitated further intervention, leading to the performance of a THR.
Discussion: This case underscores the challenges and complexities associated with managing central hip dislocation and ipsilateral knee dislocation with multiple fractures. The post-operative instability of the knee, diagnosed as an avulsion fracture of the PCL and complete ACL tear, necessitated additional intervention. The patient subsequently underwent PCL reconstruction using a semitendinosus graft, highlighting the importance of a comprehensive approach to address the diverse musculoskeletal injuries resulting from high-impact trauma.
Conclusion: The successful management of central hip dislocation and ipsilateral knee dislocation with associated fractures requires a multidisciplinary approach, incorporating timely surgical intervention, rigorous rehabilitation, and vigilant post-operative monitoring to address potential complications. This case emphasizes the need for ongoing clinical assessment and imaging studies to identify and manage secondary injuries that may manifest during the recovery phase. In addition, it highlights the development of femoral head AVN, ultimately leading to the necessity for THR.
Keywords: Musculoskeletal injury, polytrauma, comprehensive management.
Traumatic injuries resulting from road traffic accidents are characterized by their complexity, necessitating a meticulous and multidisciplinary approach to effective management. This case report delves into the detailed evaluation and operative intervention for a patient who endured a central hip dislocation, ipsilateral knee dislocation, fractures involving the lateral condyle of the left tibia and patella, and a multiligament injury to the knee following a severe road traffic accident [1]. The rarity of central hip dislocations, especially when coupled with ipsilateral knee dislocations and additional fractures, adds a layer of complexity to this case. Central hip dislocations are infrequent and typically result from high-energy trauma, making their occurrence alongside knee dislocations and fractures a rare and challenging scenario [2]. This rarity underscores the need for a thorough understanding of the mechanisms and patterns of injury, which is crucial for the development of a tailored surgical strategy. In this specific case, the injuries resulted from a severe road traffic accident, indicating a high-impact force. The combination of central hip dislocation, ipsilateral knee dislocation, and fractures in the left tibia and patella suggest a complex pattern of trauma. Addressing such intricacies requires a comprehensive evaluation of the patient, involving various imaging studies such as X-rays, computed tomography scans, and possibly magnetic resonance imaging (MRI), to fully delineate the extent and nature of the injuries [2]. The operative intervention for this multifaceted case was comprehensive, addressing each aspect of the injuries with precision. The reduction of the central hip dislocation involved careful manipulation and alignment, often requiring an open reduction approach due to the severity of the injury [3, 4]. Simultaneously, the ipsilateral knee dislocation was addressed through meticulous reduction and stabilization procedures [5]. Attention to the fractures in the lateral condyle of the left tibia and patella involved conservative management. Following the initial operative intervention, the second stage was dedicated to managing the multi-ligament injury to the knee. This phase involved a detailed assessment of ligamentous structures, potentially utilizing grafts for reconstruction, and implementing surgical techniques to restore stability and function to the knee joint. The staged approach allowed for a thorough and systematic management of each aspect of the complex injuries, minimizing the risk of complications and optimizing long-term outcomes [6]. Post-operative care and rehabilitation play a crucial role in the overall management of such cases. Close monitoring for complications, including infection or vascular compromise, is essential. A structured rehabilitation program, encompassing physiotherapy and occupational therapy, is initiated to promote optimal recovery, restore functionality, and prevent long-term disability. Following the successful operative and rehabilitation phases, it was observed that the femoral head had developed avascular necrosis (AVN). This complication necessitated further intervention, leading to the performance of a total hip replacement (THR). Managing a patient with central hip dislocation, ipsilateral knee dislocation, fractures involving the tibia and patella, and a multi-ligament knee injury presents unique challenges. Complications such as post-operative stiffness, joint instability, or neurovascular compromise may arise, necessitating vigilant post-operative care, and prompt intervention if necessary. Effective communication and coordination among the healthcare team are vital to navigate unforeseen challenges successfully [7].
A 28-year-old male presented to the emergency department after a high-impact road traffic accident. Clinical examination and radiographic imaging revealed a complex array of injuries, including central hip dislocation, ipsilateral knee dislocation (Schenck Classification -KD V) [8], and fractures of the lateral condyle of the left tibia and the patella (Fig. 1-4).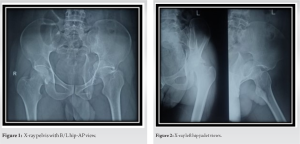
Urgent operative intervention was initiated to address the intricate musculoskeletal injuries. Closed reduction and internal fixation with K-wires were employed to manage knee dislocation (Fig. 5). Simultaneously, open reduction utilizing a 9-hole RECON plate was performed to address the central hip dislocation (Fig. 6, 7).
Simultaneously, open reduction utilizing a 9-hole RECON plate was performed to address the central hip dislocation (Fig. 6, 7).
Lateral condyle fracture and patella fracture were managed conservatively.

Postoperatively, a long leg slab was applied for 6 weeks to facilitate optimal healing and stability. Following the immobilization period, K-wires were removed (Fig. 8), and the patient initiated physiotherapy with partial weight-bearing permitted.
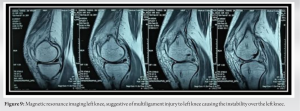
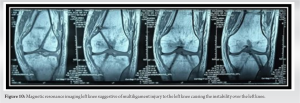
Despite the initial success of the operative interventions, several weeks into the post-operative recovery phase, the patient reported persistent instability over his left knee during weight-bearing activities. An MRI investigation was subsequently conducted, revealing an avulsion fracture of the posterior cruciate ligament (PCL) from its tibial attachment site and a complete anterior cruciate ligament (ACL) tear (Fig. 4) which was managed 6 months after sustaining injury with arthroscopic ACL and PCL reconstruction using semitendinosus and gracilis grafting (Fig. 9, 10).
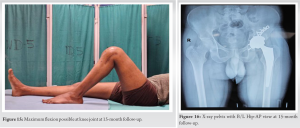
On closer examination of the hip, unforeseen complications emerged. The femoral head displayed signs of AVN 9 months after sustaining an injury, a condition attributed to the high-impact trauma sustained in the road traffic accident. This development was confirmed through X-ray (Fig. 11, 12), shedding light on the underlying cause of the persistent issues in the post-operative phase. Recognizing the severity of the AVN in the femoral head and its potential long-term consequences, the medical team decided to proceed with a THR (Fig. 13). This surgical intervention aimed to alleviate pain, restore joint function, and address the necrotic changes within the hip joint by replacing the compromised joint with an artificial implant. At the last follow-up visit (15 months after sustaining the injury), the patient’s hip and knee movements were assessed. Movement at the hip joint was completely satisfactory, whereas there was 20° restriction in flexion at the knee joint (Fig. 14-16).


The presented case involves a 35-year-old male who experienced a high-impact road traffic accident, resulting in complex musculoskeletal injuries, including central hip dislocation, ipsilateral knee dislocation, and fractures of the lateral condyle of the left tibia and patella. The comprehensive operative management employed a combination of closed reduction and internal fixation for the tibial and patellar fractures and open reduction with a 9-hole RECON plate for the central hip fracture-dislocation. The subsequent post-operative period included immobilization with a long leg slab for 6 weeks, followed by the initiation of physiotherapy and partial weight-bearing. However, a noteworthy complication emerged during the rehabilitation phase. The patient reported instability over his left knee, prompting further investigation through MRI. The MRI findings disclosed an avulsion fracture of the PCL and a complete ACL tear, emphasizing the complexity and multilayered nature of the initial trauma. In addition, the femoral head was found to have developed AVN, a condition likely stemming from the high-impact trauma [9]. The avulsion fracture of the PCL and complete ACL tear observed in this case are indicative of the significant forces applied to the knee during the traumatic incident. Such injuries can lead to persistent instability and may compromise the long-term function of the knee joint. The management of ligamentous injuries often involves a combination of surgical intervention and physiotherapy to restore stability and function. The development of AVN in the femoral head is a severe complication that can arise from disruption of the blood supply due to trauma. In this case, the high-impact nature of the road traffic accident likely led to compromised blood flow to the femoral head, resulting in ischemic necrosis. AVN can have profound implications for joint health, causing pain, and dysfunction and necessitating further surgical intervention. Given the extent of AVN in the femoral head and recognizing its potential impact on the patient’s mobility and quality of life, the decision was made to perform a THR [10]. THR is a well-established surgical intervention for end-stage hip pathology, offering relief from pain and restoration of joint function through the replacement of the damaged joint with an artificial implant.
This complex case highlights the challenges following high-impact trauma. While initial surgery addressed fractures, unforeseen complications arose during rehablitation. Ligament tears in the knee and AVN in the hip emerged, showcasing the potential for hidden injuries and systemic consequences. To address these issues, a multidisciplinary approach with close monitoring and further interventions, like THR, proved crucial for optimizing the patient’s long-term joint health and function.
Management of complex musculoskeletal trauma involving central hip dislocation and ipsilateral knee dislocation necessitates a comprehensive approach. This includes not only initial surgical intervention for fractures but also ongoing monitoring, rehabilitation, and potential additional procedures like ACL reconstruction and THR to address unforeseen complications. A multidisciplinary team is essential for successful long-term management of these complex injuries.
References
- 1.Alho A. Injuries in the femoral axis. Int Orthop 1980;3:271-9. [Google Scholar]
- 2.Sharma G, Chahar D, Sreenivasan R, Verma N, Pankaj A. Ipsilateral hip and knee dislocation: Case report and review of literature. J Clin Orthop Trauma 2016;7:115-21. [Google Scholar]
- 3.Lewis SR, Macey R, Lewis J, Stokes J, Gill JR, Cook JA, et al. Surgical interventions for treating extracapsular hip fractures in older adults: A network meta-analysis. Cochrane Database Syst Rev 2022;2:CD013405. [Google Scholar]
- 4.Chen CY, Hsu CJ, Lin TL, Chen HT, Tsai CH. Acetabular fractures with central hip dislocation: A retrospective consecutive 50 case series study based on AO/OTA 2018 classification in midterm follow-up. Biomed Res Int 2021;2021:6659640. [Google Scholar]
- 5.Kupczik F, Schiavon ME, Vieira LD, Tenius DP, Fávaro RC. Knee Dislocation: Descriptive study of injuries. Rev Bras Ortop 2013;48:145-51. [Google Scholar]
- 6.Li T, Xiong Y, Zhang Z, Tang X, Chen G, Li Q, et al. Results of multiple ligament reconstruction after knee dislocation--A prospective study with 95 patients and minimum 2-year follow up. BMC Musculoskelet Disord 2021;22:904. [Google Scholar]
- 7.Konarski W, Poboży T, Śliwczyński A, Kotela I, Krakowiak J, Hordowicz M, et al. Avascular necrosis of femoral head-overview and current state of the art. Int J Environ Res Public Health 2022;19:7348. [Google Scholar]
- 8.Goebel CP, Domes C. Classifications in brief: The schenck classification of knee dislocations. Clin Orthop Relat Res 2020;478:1368-72. [Google Scholar]
- 9.Guan NJ, Myint Y, Ali FM. Management of multiligament knee injuries. EFORT Open Rev 2020;5:145-55. [Google Scholar]
- 10.Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury 2015;46:484-91. [Google Scholar]








