
Wide resection combined with extensor carpi ulnaris (ECU) tenodesis is an effective approach for treating huge giant cell tumors (GCTs) in the distal ulna, leading to improved wrist function and reduced recurrence rates.
Dr. Suhas Aradhya BM, Department of Orthopaedics, All India Institute of Medical Sciences, Nagpur, Maharashtra, India. E-mail: suhas.aradhya143@gmail.com
Introduction: Giant cell tumors (GCT) are a relatively uncommon type of non-cancerous bone growth, representing around 4–10% of all bone tumors. These tumors tend to exhibit local aggressiveness and are typically prevalent in individuals between 20 and 40 years old. Commonly observed locations for GCT include the distal femur, proximal tibia, and the distal end of the radius. However, occurrences at the distal end of the ulna are rare, accounting for only 0.45–3.2% of cases.
Case Report: In this instance, we present the case of a 36-year-old male diagnosed with a GCT specifically located in the left distal ulna. Our approach involved managing the patient through the complete removal (en-bloc resection) of the distal ulna. Following this, we performed an extensor carpi ulnaris (ECU) tenodesis to stabilize the proximal stump. After 2-year follow-up, the patient exhibited positive outcomes, displaying satisfactory wrist joint mobility and functionality without any signs of tumor recurrence.
Conclusion: This case emphasizes the effectiveness of wide resection as a viable treatment for huge GCTs in the distal ulna. Utilizing tenodesis with the tendon of ECU significantly contributes to stabilizing the ulnar stump, leading to improved wrist function.
Keywords: Giant cell tumor, distal ulna, en-bloc resection, extensor carpi ulnaris tenodesis, recurrence.
A giant-cell tumor (GCT) is a rare, non-cancerous bone tumor known for its local invasiveness. It is not very common, accounting for roughly 4–10% of all bone tumors, typically affecting individuals aged between 20 and 55 years [1]. This tumor usually appears in the meta-epiphyseal region of long bones of young adults [1]. Commonly, it is found in the distal femur and proximal tibia, followed by the distal end of the radius [2]. However, occurrence in the distal end of the ulna is exceptionally rare, representing only about 0.45–3.2% of all cases of GCTs [3]. Since the main mechanical pivot point in the wrist is the radiocarpal joint, the lower end of the ulna bone can be considered somewhat dispensable [4]. Removing this part of the ulna may result in an acceptable decrease in functionality [4]. Darrach was the first to discuss removing the lower end of the ulna to correct deformities after injuries [5]. Since then, various modifications to this procedure have been proposed. There is debate among experts about whether the removed ulna should be stabilized. Some argue against any form of reconstruction, while others prefer different methods of stabilizing the area [6]. We present a unique case of distal Ulna GCT where we managed with wide local excision and extensor carpi ulnaris (ECU) tenodesis.
A 36-year-old man from India came in with pain and swelling on the inner side of his left lower forearm that had been bothering him for 10 months. There was no history of trauma. Initially, he received basic care and pain-relieving medications at a private clinic. He did not report any other significant symptoms apart from the localized discomfort and swelling. His personal, work, and medical backgrounds did not reveal anything noteworthy. On examination, there was a smooth oval-shaped swelling measuring 8 × 6 cm approximately on the medial aspect of the left distal forearm (Fig. 1). The skin over this swelling appeared normal without any scars, openings, or prominent veins. The swelling felt tender to the touch and had a firm consistency. There was mild local rise of temperature over the area. Movement in the left wrist joint as well as pronation and supination of the left forearm was restricted compared to the opposite side, both actively and passively. However, there were no distal neurovascular deficits.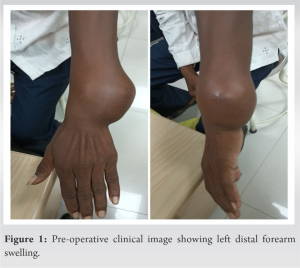
Further examination through an X-ray of the forearm with wrist revealed a lytic lesion within the left distal ulna. The bone showed signs of expansion and ballooning in its structure and without any periosteal reaction (Fig. 2a).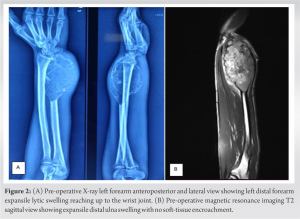
The magnetic resonance imaging scans revealed a bone lesion in the lower part of the ulna bone, displaying an expansile lytic nature (Fig. 2b). This lesion showed irregularities in the bone’s outer layer, extending toward the joint surface of the wrist. However, there was no soft tissue or neurovascular involvement. Based on clinical and radiological observations, a diagnosis of GCT was suspected. A core needle biopsy was conducted to confirm this diagnosis which showed mononuclear stromal cells and uniformly distributed multinucleated giant cells. Mononuclear stromal cells have oval to spindle-shaped nuclei with moderate cytoplasm. The intermixed giant cells show a variable number of nucleoli (usually >20 nucleoli). Few bony trabeculae and muscle tissue seen. Mitosis or necrosis was not seen. Findings are suggestive of GCT of bone (Fig. 3).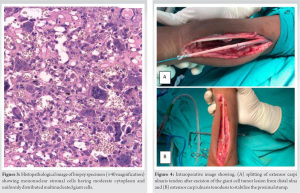
The patient was operated with wide local excision of distal ulna and ECU tenodesis for stabilization (Fig. 4). The excised mass was lobulated in appearance (Fig. 5).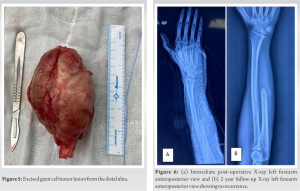 Patient was kept on an above elbow slab support for 14 days and then sutures removed after that. Elbow and wrist range of motion exercises were started. The patient was followed up regularly both clinically and radiologically for 2 years (Fig. 6 and 7). Two years later, assessment revealed that the patient exhibited excellent wrist and forearm movement, a strong grip, and no signs of instability or tumor recurrence. There was also no radiological evidence of recurrence at the end of 2 years.
Patient was kept on an above elbow slab support for 14 days and then sutures removed after that. Elbow and wrist range of motion exercises were started. The patient was followed up regularly both clinically and radiologically for 2 years (Fig. 6 and 7). Two years later, assessment revealed that the patient exhibited excellent wrist and forearm movement, a strong grip, and no signs of instability or tumor recurrence. There was also no radiological evidence of recurrence at the end of 2 years.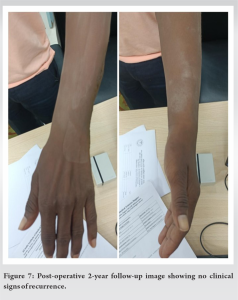
GCT is a rare benign bone tumor that typically manifests in individuals aged 20–40 years [1]. Its occurrence in the distal end of the ulna is infrequent, with an incidence rate ranging from 0.45–3.2% [3]. The primary aim of treatment is complete removal of the affected area with safe margins, alongside reconstruction and stabilization of the ulnar stump to prevent recurrence and preserve joint function. The literature showcases diverse treatment options available for GCTs in the ulna, spanning from extended curettage with bone grafting or cementation to wide resection, sometimes involving reconstruction with allografts, prostheses, or bone transport using Ilizarov techniques [7]. For small lesions, extended curettage is commonly used. However, some studies advocate the recurrence rate of curettage alone (40%) [8]. Adequate tumor removal is emphasized as a crucial factor in the surgical outcome. Bigger lesions are often managed with wide resection of the ulna [9]. Various reconstruction options after ulna resection include allograft, prostheses, or Ilizarov bone transport [7]. However, these methods have limitations such as the need for bone bank facilities, time consumption, and limited availability or potential complications of prostheses. Verma et al. managed a similar case of distal ulna GCT by en-bloc resection of distal ulna along with reconstruction of distal radioulnar joint and triangular fibro cartilage complex using proximal fibula graft and palmaris longus graft [3]. Resection of the distal ulna followed by stabilization of the ulnar stump with ECU tenodesis is an alternative approach [10]. Cases described by authors like Mujaddid et al. [11] and Solichin et al. [12] suggested wide local excision with ECU stabilization. We decided to manage our case with en-bloc tumor removal and ECU tenodesis to stabilize the proximal ulna stump. After 2-year follow-up, it yielded favorable functional results with no recurrence.
The management of distal ulna GCTs remains a challenge due to their rarity and potential for recurrence. This case report highlights the effectiveness of wide resection combined with ECU tenodesis in treating huge GCTs in the distal ulna. The successful outcome, demonstrated by improved wrist function and reduced recurrence rates after a 2-year follow-up, underscores the importance of this surgical approach. Orthopedic practitioners should consider this approach in similar cases for optimal patient outcomes. This case contributes to the existing literature on the treatment of GCTs in rare locations, emphasizing the significance of prompt diagnosis and appropriate surgical intervention for improved patient management and outcomes.
This case report sheds light on the rare occurrence of GCTs in the distal ulna, emphasizing the importance of prompt diagnosis and appropriate surgical intervention. Orthopedic practitioners can benefit from understanding the distinct characteristics and treatment approaches for GCTs in this location, aiding in improved management and outcomes for affected patients.
References
- 1.Mavrogenis AF, Igoumenou VG, Megaloikonomos PD, Panagopoulos GN, Papagelopoulos PJ, Soucacos PN. Giant cell tumor of bone revisited. SICOT J 2017;3:54. [Google Scholar]
- 2.Maravi DS, Uikey S, Gaur S. Giant cell tumour of distal end radius: Various treatment protocol and results. Orthop J M P Chapter 2015;21:41-9. [Google Scholar]
- 3.Verma A, Goyal D, Patel Y. Giant cell tumor of distal ulna - a rare case report. J Orthop Case Rep 2022;12:72-4. [Google Scholar]
- 4.Helms JT, Maldonado KA, Burns B. Anatomy, shoulder and upper limb, hand radiocarpal joint. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539744 [Last accessed on 2024 Apr 09]. [Google Scholar]
- 5.Darrach W. Partial excision of lower shaft of ulna for deformity following Colles’s fracture. 1913. Clin Orthop 1992;275:3-4. [Google Scholar]
- 6.Papanastassiou ID, Savvidou OD, Chloros GD, Megaloikonomos PD, Kontogeorgakos VA, Papagelopoulos PJ. Extensor carpi ulnaris tenodesis versus No stabilization after wide resection of distal ulna giant cell tumors. Hand (N Y) 2019;14:242-8. [Google Scholar]
- 7.Burke CS, Gupta A, Buecker P. Distal ulna giant cell tumor resection with reconstruction using distal ulna prosthesis and brachioradialis wrap soft tissue stabilization. Hand (N Y) 2009;4:410-4. [Google Scholar]
- 8.Vanni D, Pantalone A, Andreoli E, Caldora P, Salini V. Giant cell tumor of the distal ulna: A case report. J Med Case Rep 2012;6:143. [Google Scholar]
- 9.Sharma V, Sharma K, Sharma S, Kanwar S, Soni RK, Katoch P. Resection and stump stabilization in giant cell tumor distal ulna: A case report. J Orthop Case Rep 2020;10:45-8. [Google Scholar]
- 10.Breen TF, Jupiter JB. Extensor carpi ulnaris and flexor carpi ulnaris tenodesis of the unstable distal ulna. J Hand Surg 1989;14:612-7. [Google Scholar]
- 11.Mujaddid I, Pamudji U, Savero I, Handry T, Brian W. Wide resection giant cell tumor of distal ulna and stabilization ulnar stump with extensor carpi ulnaris tendon (2 case reports). Int J Surg Case Rep 2020;74:58-62. [Google Scholar]
- 12.Solichin I, Martika W, Wikanjaya R. Giant cell tumor of distal ulna treated using en-bloc resection combined with extensor carpi ulnaris and flexor carpi ulnaris tendon stabilization: A case report. Int J Surg Case Rep 2021;79:362-7. [Google Scholar]






