This case emphasizes the rare occurrence of primary tuberculosis in the greater trochanter, advocating for precise diagnosis through advanced imaging. It also underscores the importance of comprehensive tuberculosis testing, particularly in extrapulmonary cases which are prevalent in developing nations, to improve treatment outcomes.
Dr. Ankita Baharani, Department of Radiology, TNMC and BYL Nair Charitable Hospital, Mumbai, Maharashtra, India. E-mail: ankitabaharani@gmail.com
Introduction: Tuberculosis (TB) of the greater trochanter constitutes about 2% of musculoskeletal TB cases, often presenting with non-specific symptoms of localized pain, tenderness, and swelling, necessitating differentiation from other conditions like tumors. Bursal involvement results in the formation of a fluctuating mass. This case emphasizes the need for meticulous diagnostic evaluation in these cases due to their uncommon presentation and potential for inadequate assessment.
Case Report: A 50-year-old male experienced hip pain and swelling after a trivial fall, leading to surgery for suspected abscess. Despite initial treatment, symptoms persisted which on further imaging suggested TB osteomyelitis that was confirmed on biopsy, prompting 18 months of anti-tubercular therapy. The patient showed significant improvement after a year, highlighting the importance of thorough evaluation and appropriate management in such cases.
Conclusion: This case emphasizes the rare occurrence of primary TB in the greater trochanter, advocating for precise diagnosis through advanced imaging. It also underscores the importance of comprehensive TB testing, particularly in extrapulmonary cases which are prevalent in developing nations, to improve treatment outcomes.
Keywords: Tuberculosis, greater trochanter, computed tomography-guided biopsy, anti-tubercular drugs.
In developed nations, bone and joint tuberculosis (TB) comprise around 2.2–4.7% of all TB instances, with approximately 10–15% categorized as extrapulmonary TB [1]. Greater trochanter TB represents about 2% of all musculoskeletal TB cases [2]. The disease typically reaches the trochanter through hematogenous spread. Patients commonly exhibit prolonged lateral hip pain, sometimes accompanied by a limp. In advanced cases, the hip joint may become involved [3]. The clinical manifestation of greater trochanter TB often lacks specificity and clarity, necessitating differentiation from tumors and other infections [4]. It is common for the bursae surrounding the trochanter to be affected, resulting in the formation of a fluctuating mass containing serum and degraded debris [5]. Potential differential diagnoses for this condition include tumors, septic bursitis, idiopathic bursitis, and osteochondritis adding to the diagnostic dilemma and definitive management [6]. Here, we present a case that highlights an unusual manifestation of primary greater trochanter TB, emphasizing the need for comprehensive diagnostic assessment due to its rarity and frequently inadequate evaluation and differentiating it from other causes affecting the greater trochanter.
A 50-year-old has a history of trivial fall at home leading to pain and localized swelling over the lateral aspect of the right hip associated with mild tenderness over a few days. The patient also developed a fever, and hence, the patient was operated with incision and drainage over the swelling, suspecting a post-traumatic abscess. The collection was sent for only bacterial staining and culture sensitivity, which was inconclusive, and started on empirical antibiotics for 4 weeks. The patient was asymptomatic for 10 months, after which he developed pain at the same site associated with difficulty on weight bearing and walking on uneven surfaces. He visited a doctor, and radiographs were advised. Based on the radiographs, a diagnosis of right old united greater trochanter fracture was made, which was managed using analgesics and anti-inflammatory drugs and asked to be followed up (Fig. 1).

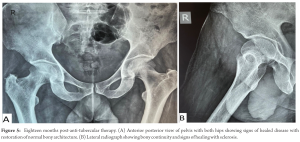
Patient continued to has symptoms for the next 2 years, which gradually worsened, and was referred to a tertiary care center. Fresh radiographs of both hips were taken for comparison, revealing sclerotic changes and osseous destruction of the greater trochanter (Fig. 2).
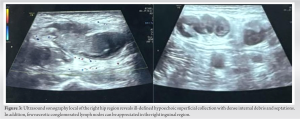
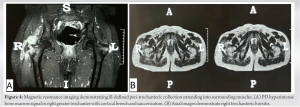
Following this, a metabolic and infective workup showed a significant elevation of C-reactive protein and erythrocyte sedimentation rate levels, indicating an inflammatory or infective condition. A local ultrasound detected a collection of twenty cubic centimeters with moving internal echoes and thin septations, raising suspicion of chronic pyogenic osteomyelitis secondary to previous surgery. However, due to the additional finding of necrotic inguinal lymph nodes, a differential diagnosis of TB osteomyelitis was also considered (Fig. 3) Further, imaging with MRI was done which revealed low signal intensity material within the fluid-filled bursa on T2-weighted images, thickened synovium appearing T2 hypointense, and necrotic right inguinal lymphadenopathy, suggesting a TB etiology rather than a pyogenic one (Fig. 4) A computed tomography (CT)-guided biopsy of the greater trochanter bone yielded negative results for CBNAAT but a positive culture for Mycobacterium tuberculosis after 6 weeks.
Consequently, a plan for conservative medical management was devised, initiating oral anti-tubercular chemotherapy for 18 months with monthly follow-ups to monitor progress. After 1 year, the patient exhibited significant clinical and radiological improvement (Fig. 5), demonstrating good adherence to treatment and physical therapy, resulting in restoration of range of motion at the hip joint and a return to normal gait and daily activities.
Musculoskeletal system is involved in 1–3% of patients of TB [7]. Hip is the 2nd most common site of TB involvement after spine. In the hip, the primary involvement of the greater trochanter and its bursa is the rarest; however, TB bursitis occurs most commonly around the hip [8]. There is no predilection for any particular age group or sex. The disease is usually multifocal though rarely; it may affect only the greater trochanter and its bursa. Ahern in 1958 described 32 patients of greater trochanter TB where the common presentation was pain, swelling, and sinus. Radiological presentation, in these cases, was in the form of erosion, cavity, and sequestrum of greater trochanter [9]. Abdelmoula et al. in 2005 described three case reports of trochanteric TB which were managed medically [10]. Mahmoud et al. in 2017 described five cases of trochanteric TB in which time to diagnosis was long (7.6 months on average); however, all cases were managed with medical treatment alone [11]. Clinical presentation is non-specific which explains the delay in diagnosis. In our case, the patient had a history of trivial trauma following which swelling developed over right hip, for which the patient underwent incision and drainage. Pus was aspirated and sent for only bacterial staining and culture which revealed negative results. All imaging modalities can help point toward the diagnosis even when initial cultures are negative. On plain radiographs, greater trochanter TB usually presents as bone destruction. In addition, wall of the distended bursa may contain calcifications, which may be appreciated. CT is better in evaluating the degree of bone destruction, sequestrum formation, and surrounding soft-tissue extension. MRI is particularly useful in early diagnosis and is the imaging investigation of choice. Low signal intensity material within the fluid-filled bursa on T2W images and adjacent abscesses is due to the presence of caseous necrosis and fibrotic material suggesting TB involvement [12], whereas hyperintensity on T2-weighted image at the abscess wall is a significant predictor of bacterial pyomyositis [13]. Synovium was also of relatively low signal intensity on T2W images. In addition, in our case, necrotic right inguinal lymphadenopathy was present which further pointed toward the diagnosis. Marrow edema in the greater trochanter was present appearing PD hyperintense; however, no marrow replacement by soft tissue was noted to suggest neoplastic involvement. Furthermore, MRI is better for the evaluation of soft-tissue extent and assessment of intra-osseous and intra-articular disease [12]. The differential diagnoses include tumor, septic bursitis, chronic pyogenic osteomyelitis, and idiopathic trochanteric bursitis [6]. The definitive diagnosis is based on bacteriological and/or histological findings, that is, culture of tubercle bacillus, synovial, and bone biopsy. In this case, a CT-guided bone biopsy of the greater trochanter was performed. GeneXpert was negative; however, culture for TB was positive. Treatment of trochanteric TB is mainly medical and based on anti-TB drugs. Our patient has had anti-TB drugs for 18 months. Combined chemotherapy alone can eradicate the disease at any stage; however, surgery is indicated in complicated cases [14]. Symptomatic improvement and healing were obtained in our case with medical treatment alone.
This case underscores the uncommon manifestation of primary TB affecting the greater trochanter, emphasizing the necessity for keen diagnostic observation and differentiation through advanced imaging to determine appropriate management strategies. In addition, it aims to raise awareness about the importance of thorough TB testing, particularly in extrapulmonary locations, given its endemic prevalence in developing nations, ultimately aiming for more favorable treatment outcomes.
This case highlights the unusual presentation of primary TB in the greater trochanter. It emphasizes the need for careful diagnosis using advanced imaging to guide treatment decisions effectively. Furthermore, it underscores the importance of thorough TB testing, especially in extrapulmonary sites, due to its common occurrence in developing countries. Ultimately, the goal is to improve treatment outcomes through heightened awareness and early detection.
References
- 1.Yoon HJ, Song YG, Park WI, Chol JP, Chanh KH, Kim JM. Clinical manifestations and diagnosis of extrapulmonary tuberculosis. Yonsei Med J 2004;45:453-61. [Google Scholar]
- 2.Babhulkar S, Pande S. Tuberculosis of the hip. Clin Orthop Relat Res 2002;398:93-9. [Google Scholar]
- 3.Tuli SM, editor. Tuberculosis of the hip joint. In: Tuberculosis of the Skeletal System (Bones, Joints, Spine and Bursal Sheaths). 3rd ed. New Delhi, India: Jaypee Brothers; 2004. p. 67-107. [Google Scholar]
- 4.Lynch AF. Tuberculosis of the greater trochanter. A report of eight cases. J Bone Joint Surg Br 1982;64:185-8. [Google Scholar]
- 5.Meyerding HW, Mroz RJ. Tuberculosis of the greater trochanter. J Am Med Asssoc 1933;101:1308-13. [Google Scholar]
- 6.Sastre S, Garcia S, Soriano A. Reactivation of ancient trochanteric tuberculosis 60 years after surgical drainage. Rheumatology (Oxford) 2003;42:1263-4. [Google Scholar]
- 7.Hugosson C, Nyman RS, Brismar J, Larsson SG, Lindahl S, Lundstedt C. Imaging of tuberculosis. V. Peripheral osteoarticular and soft-tissue tuberculosis. Acta Radiol 1996;37:512-6. [Google Scholar]
- 8.Abdelwahab IF, Bianchi S, Martinoli C, Klein M, Hermann G. Atypical extraspinal musculoskeletal tuberculosis in immunocompetent patients: Part II, tuberculous myositis, tuberculous bursitis, and tuberculous tenosynovites. Can Assoc Radiol J 2006;57:278-86. [Google Scholar]
- 9.Ahern RT. Tuberculosis of the femoral neck and greater trochanter. J Bone Joint Surg 1958;40-B:406-19. [Google Scholar]
- 10.Mahmoud I, Gafsi L, Saidane O, Souayah A, Tekaya R, Sahli H, et al. Clinical and diagnostic features of trochanteric tuberculosis. Bull Soc Pathol Exot 2017;110:242-6. [Google Scholar]
- 11.Abdelmoula LC, Chaabouni L, Ben Hadj Yahia C, Montacer Kchir M, Zouari R. Tuberculosis of the greater trochanter: A report of three cases. Joint Bone Spine 2005;72:427-9. [Google Scholar]
- 12.De Backer AI, Vanhoenacker FM, Sanghvi DA. Imaging features of extraaxial musculoskeletal tuberculosis. Indian J Radiol Imaging 2009;19:176-86. [Google Scholar]
- 13.Thammaroj P, Panitchote A, Muktabhant C, Chowchuen P. Discrimination between tuberculous and bacterial pyomyositis in magnetic resonance features. Eur J Radiol Open 2020;7:100214. [Google Scholar]
- 14.Soro Marín S, Sanchez Trenado MA, Minguez Sanchez MD, Paulino Huertas M, García Morales PV, Salas Manzanedo V. Trochanteric bursitis due to tuberculosis in an immunocompetent young woman. Reumatol Clin 2012;8:34-5. [Google Scholar]