
Dorsal scapular osteochondromas are quite rare. Diagnosis is made through a combination of imaging and histopathological examination. Asymptomatic lesions can be treated conservatively but surgical intervention is required in cases where the patient is symptomatic or malignant transformation is present.
Dr. Ayush Berwal, Department of Orthopaedics, Mahatma Gandhi Medical College and Hospital, Sitapura Industrial Area, Jaipur, Rajasthan, India. E-mail: drayushkumar@gmail.com
Introduction: Osteochondromas are a unique group of benign bone tumors that are characterized by bony outgrowth covered by Cartilage. It has a peculiar micro-architecture as its cortices are extensions of those of parent bone and there is a continuity of medullary cavity; this is akin to branching in plants, rightly earning the name “Exostosis.”
Case Report: We report a case of a 21-year-old male who presented with complaints of swelling on the upper back associated with mild discomfort. Examination confirmed a bony mass on the dorsal aspect of the scapula without any restricted range of motion of the shoulder joint. On the confirmation of diagnosis, en bloc excision was performed.
Conclusion: In conclusion, dorsal scapular osteochondromas are a rarity, and excision of the lesion is an effective management for symptomatic lesions.
Keywords: Osteochondroma, exostosis, scapula, orthopedic tumor.
Osteochondroma, as an orthopedic entity sits tightly on the fence between neoplastic and non-neoplastic lesions. Although considered as a benign bone tumor, it represents a developmental aberration involving ectopic migration of a part of the growth plate and its autonomous proliferation [1]. The lesion consists of a bony mass and overlying cartilage, with its cortex and medullary cavity contiguous with those of the originating bone. Its growth also mirrors the growth of its parent bone and peaks at skeletal maturity, unless it transforms into a malignant lesion [2, 3]. It is mostly found as a solitary lesion but may present as multiple lesions in a condition known as multiple hereditary exostoses [4, 5]. Owing to its asymptomatic nature, it is usually found incidentally on imaging or occasionally presents as a painless lump. Rarely, it might present with pain because of mechanical irritation of adjacent structures including muscles and tendons, or if there is a malignant transformation of the lesion [6, 7]. The distal femur, proximal tibia, and proximal humerus constitute the most common sites of presentation of osteochondroma [8]. The scapula is a relatively rare site, but osteochondroma is the most common tumor of the scapula. Most scapular osteochondromas present on the ventral aspect, with the dorsal side relatively less involved and less reported [9-12]. We report a case of large dorsal scapular osteochondroma in a young male.
A 21-year-old young adult presented with a swelling over the right upper thoracic region. The swelling was first noticed by the patient around 9 years ago, as a peanut-sized lump which progressively grew to about the size of a golf ball at the present day. There was no history of any significant trauma or any other lump. It was painless for the majority of its duration but started causing discomfort in the past 2 months before the presentation. Due to its asymptomatic nature for much of the course, the patient avoided any surgical treatment advised to him multiple times. On examination, the swelling was solitary, protuberant, localized, spherical, and non-pulsatile. The overlying skin was unremarkable and there was no change in local skin temperature. Swelling was non-tender and globular with dimensions of 5.5 cm × 6 cm × 3.5 cm. Bony hard consistency was evident with clearly defined edges. The swelling was fixed to the underlying scapula, a few centimeters above the inferior angle. It was non-fluctuating and non-reducible. There was a movement of the swelling corresponding to the movements of the scapula. Neurovascular examination of the right upper limb was unremarkable (Fig. 1).
A biopsy sample was taken and sent for histopathological examination. The report suggested a chondroid lesion with the focal osseous component. Findings were consistent with osteochondroma without any element of sarcomatous changes.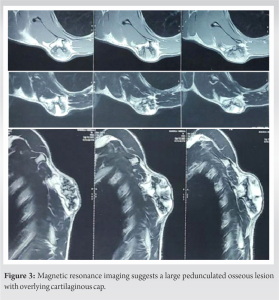
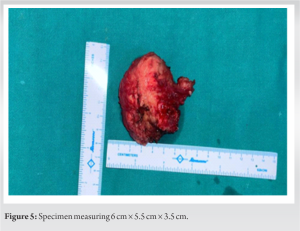
En bloc excision of the lesion was planned. The patient was taken on the operation Table 1 in a prone position under the effect of general anesthesia. A 7.5 cm incision was taken centered over the swelling and parallel to the medial margin of the scapula. The muscle was separated along the plane created by the tumor above the mass and the base of the mass was accessed from all directions. It was dissected with the periosteum and excised along with the periosteum from the base with the help of an osteotome. The specimen measured 6 cm × 5.5 cm × 3.5 cm (Fig. 4 and 5).
The patient had immediate relief postoperatively. He was called for follow-up at 15 days, 1 month, 2 months, and 3 months postoperatively and assessed clinically and functionally. There was no pain or reappearance of swelling. Shoulder range of movements and scapulo-thoracic rhythm were normal at 3 months postoperatively (Fig. 6 and 7).
Despite the common occurrence of osteochondromas, the scapula remains a relatively less common site. This can be explained by the fact that scapula ossifies through intra-membranous mode while the most acceptable paradigm of the pathogenesis of osteochondroma is the migration of growth plate remnants to an ectopic location [13, 14]. However, there is a caveat, that osteochondromas constitute the most common tumor of scapula and the most common site is the ventral surface [15-19]. Usually, they follow the growth and development of the parent bone and are present in 2nd or 3rd decade of life. They are mostly asymptomatic but may irritate adjacent structures leading to a myriad of signs and symptoms. Although plain radiography forms the gold standard imaging modality for their diagnosis, suspected osteochondromas of scapula require MRI. MRI is advised when a malignant transformation is suspected. Most asymptomatic lesions are treated conservatively but symptomatic lesions usually require surgery. Our case had a more rare presentation as the tumor was on the dorsal surface. We have also reviewed similar case reports (Table 1).
Dorsal scapular osteochondromas are a rarity. Here, we have reported a case of a 21-year-old male patient with a globular swelling on the upper back associated with discomfort. After making a diagnosis after radiological and histopathological examination, the decision of en bloc excision of the lesion was taken in view of symptoms.
A mindfully rehearsed sequence of diligent history-taking, careful clinical examination, appropriate imaging, and biopsy is required for the diagnosis of osteochondroma at a location as rare as the dorsal scapula. En bloc excision is the choice of procedure if the indications for surgery are met.
References
- 1.Milgram JW. The origins of osteochondromas and enchondromas. A histopathologic study. Clin Orthop Relat Res 1983;174:264-84. [Google Scholar]
- 2.Toy PC, Heck RK Jr. Benign bone tumors and nonneoplastic conditions simulating bone tumors. In: Azar FM, Beaty JH, editors. Campbells’s Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021. p. 965-6. [Google Scholar]
- 3.Alabdullrahman LW, Byerly DW. Osteochondroma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar]
- 4.Keith A. Studies on the anatomical changes which accompany certain growth-disorders of the human body: I. The nature of the structural alterations in the disorder known as multiple exostoses. J Anat 1920;54:101-15. [Google Scholar]
- 5.Garcia RA, Inwards CY, Unni KK. Benign bone tumors-recent developments. Semin Diagn Pathol 2011;28:73-85. [Google Scholar]
- 6.Okada K, Terada K, Sashi R, Hoshi N. Large bursa formation associated with osteochondroma of the scapula: A case report and review of the literature. Jpn J Clin Oncol 1999;29:356-60. [Google Scholar]
- 7.Jangir R, Misra D. Scapulothoracic dissociation: A rare variant: A case report. Malays Orthop J 2014;8:46-8. [Google Scholar]
- 8.de Souza AM, Bispo RZ Jr. Osteochondroma: Ignore or investigate? Rev Bras Ortop 2014;49:555-64. [Google Scholar]
- 9.Galate JF, Blue JM, Gaines RW. Osteochondroma of the scapula. Mo Med 1996;92:95-7. [Google Scholar]
- 10.Sivananda P, Rao BK, Kumar PV, Ram GS. Osteochondroma of the ventral scapula causing scapular static winging and secondary rib erosion. J Clin Diagn Res 2014;8:LD03-5. [Google Scholar]
- 11.Tittal P, Pawar I, Kapoor SK. Pseudo-winging of scapula due to benign lesions of ventral surface of scapula - two unusual causes. J Clin Orthop Trauma 2015;6:30-5. [Google Scholar]
- 12.Calafiore G, Calafiore G, Bertone C, Urgelli S, Rivera F, Maniscalco P. Osteochondroma. Report of a case with atypical localization and symptomatology. (Article in Italian). Acta Biomed Ateneo Parmense 2001;72:91-6. [Google Scholar]
- 13.Garcia SA, Ng VY, Iwamoto M, Enomoto-Iwamoto M. Osteochondroma pathogenesis: Mouse models and mechanistic insights into interactions with retinoid signaling. Am J Pathol 2021;191:2042-51. [Google Scholar]
- 14.Tepelenis K, Papathanakos G, Kitsouli A, Troupis T, Barbouti A, Vlachos K, et al. Osteochondromas: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features and treatment options. In Vivo 2021;35:681-91. [Google Scholar]
- 15.Alrashedan BS, Chowdhary SK, Mahmoud J, Hamza OM. Symptomatic osteochondroma in the ventral aspect of the scapula in a child with hereditary multiple exostoses. J Musculoskelet Surg Res 2019;3:370-3. [Google Scholar]
- 16.El Rharras S, Farah R, El Haoury H, Saidi H, El Bouchti I. Solitary osteochondroma of the scapula: An uncommon localization. Clin Case Rep Rev 2017;3:1-3. [Google Scholar]
- 17.Seth A, Naqvi M, Yadav U, Karumuri K, Annapareddy A, Reddy AV. Unveiling scapular pseudo-winging: A case report on ventral osteochondroma of the scapula in a 21-year-old. J Orthop Case Rep 2023;13:99-104. [Google Scholar]
- 18.Dharmadhikari RP. Painful snapping and pseudo-winging scapula due to a large scapular osteochondroma. J Orthop Case Rep 2012;2:10-3. [Google Scholar]
- 19.Ermiş MN, Aykut US, Durakbaşa MO, Ozel MS, Bozkuş FS, Karakaş ES. Snapping scapula syndrome caused by subscapular osteochondroma. Eklem Hastalik Cerrahisi 2012;23:40-3. [Google Scholar]
- 20.Fjeldborg PK, Hansen TB. Atypisk årsag til scapula alata på baggrund af eksostose på scapula [Atypical cause of scapular winging due to exostosis of the scapula]. Ugeskr Laeger 2012;174:354-5. [Google Scholar]
- 21.Yadkikar SV, Yadkikar VS. Osteochondroma on dorsal surface of the scapula in 11 years old child-a case report. Int J Med Res Health Sci 2013;2:305-8. [Google Scholar]
- 22.Vaishya R, Dhakal S, Vaish A. A solitary osteochondroma of the scapula. BMJ Case Rep 2014;2014:bcr2013202273. [Google Scholar]
- 23.Nekkanti S, Moogali A, Meka A, Nair M. An unusual presentation of osteochondroma on the dorsal surface of the scapula: A review of two patients. J Orthop Case Rep 2018;8:38-41. [Google Scholar]
- 24.Ngongang FO, Fodjeu G, Fon AC, Fonkoue L, Guifo ML, Bitang A Mafok LJ, et al. Surgical treatment of rare case of scapula osteochondroma in a resource limited setting: A case report. Int J Surg Case Rep 2019,61:130-4. [Google Scholar]
- 25.Shahid O, Shahid M, Shaik L, Masud M, Ranjha S. Rare case of osteochondroma on the dorsal aspect of the scapula. Cureus 2021;13:e17051. [Google Scholar]
- 26.Segura Sánchez D, Pino Almero L, Mínguez Rey MF. Osteocondroma solitario de la escápula: localización poco habitual para un tumor frecuente [A solitary osteochondroma of the scapula: Uncommon location for a common tumor]. Arch Argent Pediatr 2021;119e562-6. [Google Scholar]
- 27.Jindal V, Khandekar A, Gupta P, Binyala S. Solitary osteochondroma of the scapula in a young male: A case report. J Orthop Case Rep 2022;12:34-7. [Google Scholar]
- 28.Altwaijri NA, Fakeeha J, Alshugair I. Osteochondroma of the scapula: A case report and literature review. Cureus 2022;14:e30558. [Google Scholar]
- 29.Faur C, Abu-Awwad A, Patrascu JM Jr., Abu-Awwad SA, Tudoran C. Superomedial scapula angle osteochondroma with winging in a young female patient-case report and literature review. J Clin Med 2023;12:5106. [Google Scholar]
- 30.Das R, Arya S, Krishna A, Ghosh S, Mukartihal R, Keezhadath S. Osteochondroma of dorsal scapula: A case report and review of literature. J Orthop Case Rep 2023;13:104-9. [Google Scholar]








