
In a series of simultaneous bilateral TKR, significant improvement in the functional outcome was noted in restoring the mechanical axis to near-normal values.
Dr. Joe Joseph Cherian, Department of Orthopaedics, St Johns Medical College, Bengaluru, Karnataka, India. E-mail: cherianjoe71@gmail.com
Introduction: Osteoarthritis (OA) is the most frequent joint disease with a prevalence of 5313/100,000 persons in India. OA of the knee is a major contributor to mobility impairment, particularly among women. In these patients, total knee replacement (TKR) is widely accepted as the gold-standard treatment for pain relief and restoration of function. Now, patients have the option of undergoing either a simultaneous bilateral TKR or a staged TKR. The former has shown significant advantages such as shorter rehabilitation, cost efficacy, and shorter hospital stay. This study aimed to assess the functional and radiological outcome of simultaneous bilateral TKR in a tertiary care center.
Materials and Methods: 30 adult patients above the age of 55 years with severe OA knee who underwent simultaneous bilateral TKR between 2022 and 2023 were included in this prospective study. Pre-operatively, they were assessed with radiographs including full-length scanograms. The mean anatomical axis, mean mechanical axis, and mechanical axis deviation (Varus) were calculated based on the scanograms by a single observer. The same observer administered the Oxford Knee Score (OKS) pre-operatively to all patients. Regular clinical and radiological follow-up was done. After 1-year follow-up, the same observer administered the OKS to the operated knee.
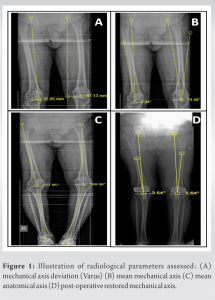
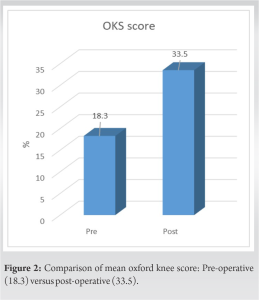
Results: With a female preponderance among the study subjects (56.7%), the majority of the cases in our cohort were characterized as Grade IV Kellgren–Lawrence radiological grade of OA (76.66%) and were found to have tricompartmental involvement (70%). The mean anatomical axis for the right and left lower limbs was 4.56 ± 5.17 and 9.68 ± 1.72, respectively. The mean mechanical axis deviation (Varus) for the right and left lower limb was 31.6 ± 15.1 and 52.0 ± 13.9, respectively. Preoperatively, the mean mechanical axis for the right and left lower limbs was 9.95 ± 4.31 and 14.2 ± 0.67, respectively. Postoperatively, the mechanical axis was restored to near-normal values (3–5°). Significant improvement in mean OKS from a pre-operative value of 18.30 ± 3.46 to the post-operative value of 33.50 ± 5.32 was noted at 1 year.
Conclusion: Treatment of severe bilateral OA knee with simultaneous single-staged bilateral TKR ensures good functional outcome and early mobility with minimal complications.
Keywords: Simultaneous bilateral total knee replacement, oxford knee score, mechanical axis deviation.
Osteoarthritis (OA), also known as degenerative arthritis, is the second most common rheumatologic problem and the most frequent joint disease with an age-standardized prevalence of 5313/100,000 persons (95% uncertainty interval: 4799–5898) in India [1]. It is a chronic degenerative condition of complex, multifactorial etiology, characterized by articular cartilage loss, subchondral sclerosis, osteophyte formation, and a variety of biochemical and morphological changes of the synovial membrane and joint capsule [2]. With its prevalence increasing dramatically with age [3], OA of the knee is a major contributor to the impairment of mobility, particularly among women [3]. For severe cases of OA knee, total knee replacement (TKR) is widely accepted as the gold-standard treatment for pain relief and restoration of function in patients with advanced degenerative OA [4]. In spite of being estimated to be among the leading causes of non-fatal burden [5], controversy exists concerning the timing of the definitive treatment for OA knee, i.e., TKR. Patients suffering from severe OA knee have the choice of undergoing either a single-stage bilateral TKR or a staged TKR, within the same or two separate hospital stays. Between the two, single-stage bilateral knee replacement has the advantage of shorter hospital stay, shorter rehabilitation, and reduced patient management costs [6]. Both prospective [7] and retrospective [6] studies have been conducted exploring single-stage bilateral TKR. Literature has shown that opting for bilateral rather than two unilateral replacements results in a reduction in expenses ranging from 18% to 50% [8]. However, there are differing views concerning complication rates with studies concluding lower [9], similar [10], and higher morbidity rates [11] compared to staged TKR. The purpose of this study was to assess the functional and radiological outcome of simultaneous single-stage bilateral TKR in a series of 30 patients, all treated at a tertiary care center with a follow-up of 1.
We conducted a prospective analysis of patients with bilateral knee OA who underwent a simultaneous bilateral knee replacement between 2022 and 2023. This study was initiated after obtaining the institution’s ethics committee’s approval. Adult patients above the age of 55 years with primary/secondary OA of the knee who underwent simultaneous bilateral TKR and had a follow-up of a minimum of 1-year post-operatively were included in the study. Patients with rheumatoid arthritis or other inflammatory arthritis and patients who underwent staged procedures were excluded from the.
Patients were assessed pre-operatively using radiographs including full-length lower limb scanograms and classified as per Kellgren–Lawrence grade [12]. The mean anatomical axis, mean mechanical axis, and mechanical axis deviation (Varus) were calculated based on the scanograms by a single observer. A single observer administered the Oxford Knee Score (OKS) [13] pre-operatively to all included patients. Regular clinical and radiological follow-up was done. At the 1-year follow-up mark, a single observer administered the OKS to the operated knee. Developed in 1998, the OKS is a primary outcome measure of choice following knee replacements [13]. It is a patient-reported outcome measure that consists of 12 questions about an individual’s level of function, activities of daily living, and how they have been affected by pain over the preceding 4 weeks. Total scores range from 0 (poorest function) to 48 (maximal function). The patients were then explained about the pros and cons of undergoing single-stage bilateral TKR and informed consent was obtained.
Surgical procedure
The surgical procedure was carried out by the same senior orthopedic surgeon. Patients were administered prophylactic injection cefuroxime (1.5 g) + sulbactam during induction of anesthesia and another dose just before the second knee incision was made. Following this, the patients received 2 more doses of antibiotic every 8th h postoperatively. All patients were operated by standard medial parapatellar approach. Soft tissue balancing and bone cuts were made using standard techniques. In all cases, cemented posterior stabilizing system was used. A bilateral pneumatic tourniquet was used in all cases. Only when the 1st knee skin was closed and the tourniquet released, the pneumatic tourniquet in the 2nd knee inflated. Hemostasis was achieved before skin closure. Preventive anticoagulant therapy with oral novel anticoagulant started within 12 h after surgery and continued for 15 days.
Post-operative protocol
Patients were started on active ankle pump and quadriceps strengthening exercises immediately following surgery. Full weight-bearing mobilization was initiated for the operated patients on post-operative day 1. Knee range of movement exercises was started on day 1. All patients included in the study achieved knee flexion of 90° and were comfortably ambulating full weight bearing by the end of 1 week postoperatively. They were discharged on day 12 after the removal of sutures.
Statistics
We used IBM SPSS (Version 20.0, Armonk, NY:IBM Corp, USA) Statistics software for the analysis of our results. Pre- and post-operative OKS were compared using paired t-test. The statistical significance value (P) was set to 0.05.
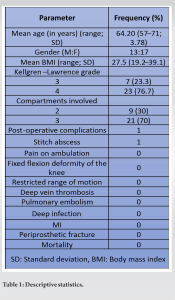
Thirty patients, who satisfied the inclusion criteria, were analyzed. The mean age at presentation was 64.2 years (range: 57–71 years; standard deviation: 3.78) with a female preponderance (17/30, 56.7%). The majority of the cases in our cohort were characterized as Grade IV Kellgren–Lawrence radiological grade of OA (23/30; 76.66%) and were found to have tricompartmental involvement (21/30; 70%) (Table 1). The mean anatomical axis for the right and left lower limbs were 4.56 ± 5.17 and 9.68 ± 1.72, respectively. The mean mechanical axis deviation (Varus) for the right and left lower limb was 31.6 ± 15.1 and 52.0 ± 13.9, respectively. Preoperatively, the mean mechanical axis for the right and left lower limbs was 9.95 ± 4.31 and 14.2 ± 0.67, respectively. Postoperatively, the mechanical axis was between 3 and 5°, according to the standard protocol (Fig. 1). The OKS was administered at variable duration for each individual but only after 1 year of the surgical procedure. There was a significant improvement in the mean OKS from a pre-operative value of 18.30 ± 3.46 to a post-operative value of 33.50 ± 5.32 at a follow-up of 1 year (Fig. 2). All the patients were examined for any post-operative complications. Of the 30 patients, 1 was noted to have a stitch abscess and 1 had persistent pain on ambulation. Patients improved with oral antibiotics, physiotherapy, and knee range of motion exercises. Not a single case of fixed flexion deformity of the knee or restricted range of motion was noted. In our study, complications such as DVT/PE, MI, deep infection, and periprosthetic fracture were not noted. There was no post-operative intensive care unit admission or mortality in our cohort.
A review of the literature over the years has shown significant benefits of a simultaneous bilateral knee replacement in terms of patient hospital stay, total cost of the treatment, and rehabilitation. In our study, we noted an increase in the mean OKS from 18.30 preoperatively to 33.5 which is statistically significant (P < 0.05). The mean duration of hospital stay in our study population was 12.03 days as per the institution’s protocol. Our results were in conjunction with a recent study carried out by Krishnamoorthy et al. [14] exploring the functional outcome of single-staged simultaneous bilateral TKR, exhibiting an improvement in OKS from 11.47 to 46.31. Hence, we found our results reassuring. In this study, none of the patients developed major complications, such as deep infection requiring secondary surgical procedures, symptomatic deep vein thrombosis/pulmonary embolism, or mortality. We had one patient with a stitch abscess which was managed medically with oral antibiotics and another with persistent pain on ambulation which improved with physiotherapy. The literature review revealed contradicting evidence regarding complications associated with simultaneous bilateral TKR. Girish Sabari et al. [15] noted an increase in the incidence of neurological complications, particularly disorientation, in the post-operative phase. However, none of the patients in our study were found to have such a complication. Acute renal injury and urinary tract infection have also been reported in a few studies but none were reported in the current study. For patients with unilateral and bilateral single-stage TKR, the perioperative death rate is comparable [16]. However, severe complications such as perioperative mortality were not observed in our study. Our research has certain limitations that must be addressed. The sample size and follow-up period of this study were limited. The relationship between the comorbidities of included patients and the functional outcome was not addressed. Further, large-scale prospective trials are vital for assessing the clinical and radiological outcome of simultaneous single-staged bilateral TKR.
Treatment of severe bilateral OA knee with simultaneous single-staged bilateral TKR ensures good functional outcomes and early mobility with minimal complications.
In a series of simultaneous bilateral TKR, significant improvement in the functional outcome was noted in restoring the mechanical axis to near-normal values.
References
- 1.Singh A, Das S, Chopra A, Danda D, Paul BJ, March L, et al. Burden of osteoarthritis in India and its states, 1990-2019: Findings from the Global Burden of disease study 2019. Osteoarthritis Cartilage 2022;30:1070-8. [Google Scholar]
- 2.Giorgino R, Albano D, Fusco S, Peretti GM, Mangiavini L, Messina C. Knee osteoarthritis: Epidemiology, pathogenesis, and mesenchymal stem cells: What else is new? An update. Int J Mol Sci 2023;24:6405. [Google Scholar]
- 3.Tekaya AB, Bouzid S, Kharrat L, Rouached L, Galelou J, Bouden S, et al. Health-related quality of life and associated factors among patients with knee osteoarthritis. Curr Rheumatol Rev 2023;19:355-61. [Google Scholar]
- 4.Postler AE, Lützner C, Goronzy J, Lange T, Deckert S, Günther KP, et al. When are patients with osteoarthritis referred for surgery? Best Pract Res Clin Rheumatol 2023;37:101835. [Google Scholar]
- 5.Ackerman IN, Buchbinder R, March L. Global Burden of Disease Study 2019: An opportunity to understand the growing prevalence and impact of hip, knee, hand and other osteoarthritis in Australia. Intern Med J 2023;53:1875-82. [Google Scholar]
- 6.Saini R, Powell J, Sharma R, Puloski S, Mahdavi S, Smith C, et al. One-stage versus 2-stage bilateral total joint arthroplasty: A matched cohort study. Can J Surg 2020;63:E167-73. [Google Scholar]
- 7.Goyal T, Azam MQ, Syed A, Paul S. Simultaneous single-stage versus two-staged bilateral total knee arthroplasty: A prospective comparative study. Int Orthop 2020;44:1305-10. [Google Scholar]
- 8.Wan RC, Fan JC, Hung YW, Kwok KB, Lo CK, Chung KY. Cost, safety, and rehabilitation of same-stage, bilateral total knee replacements compared to two-stage total knee replacements. Knee Surg Relat Res 2021;33:17. [Google Scholar]
- 9.Thiesen DM, Sobhani H, Gehrke T, Suero EM, Klatte TO, Citak M. A comparison of short term complication rate between 44 two- and 385 one-stage septic exchange arthroplasties in chronic periprosthetic joint infections. Orthop Traumatol Surg Res 2021;107:102668. [Google Scholar]
- 10.Siedlecki C, Beaufils P, Lemaire B, Pujol N. Complications and cost of single-stage vs. Two-stage bilateral unicompartmental knee arthroplasty: A case-control study. Orthop Traumatol Surg Res 2018;104:949-53. [Google Scholar]
- 11.Tuecking LR, Silligmann J, Savov P, Omar M, Windhagen H, Ettinger M. Detailed revision risk analysis after single- vs. Two-stage revision total knee arthroplasty in periprosthetic joint infection: A retrospective tertiary center analysis. Antibiotics (Basel) 2021;10:1177. [Google Scholar]
- 12.Goh GS, Schwartz AM, Friend JK, Grace TR, Wickes CB, Bolognesi MP, et al. Patients who have Kellgren-Lawrence grade 3 and 4 osteoarthritis benefit equally from total knee arthroplasty. J Arthroplasty 2023;38:1714-7. [Google Scholar]
- 13.Browne J, Lewsey L, Van Der Muelen J, Black N. Patient Reported Outcome Measures (PROMS) in Elective Surgery. Report to the Department of Health. London, UK: London School of Hygiene and Tropical Medicine; 2007. [Google Scholar]
- 14.Krishnamoorthy S, Govindaraj AB, Vivek AN, VijayKumar S, Anand M. Functional outcome of single stage bilateral total knee replacement measured using oxford knee score. J Arthrosc Jt Surg 2019;6:94-7. [Google Scholar]
- 15.Girish Sabari R, Gopalakrishnan KC, Sugath S, Anoop S. Simultaneous bilateral total knee arthroplasty - Is it the final answer? Kerala J Orthop 2011;24:15-22. [Google Scholar]
- 16.Shin YH, Kim MH, Ko JS, Park JA. The safety of simultaneous bilateral versus unilateral total knee arthroplasty: The experience in a Korean hospital. Singapore Med J 2010;51:44-9. [Google Scholar]





