The purpose of this article is to emphasize the uncommon occurrence of mid-shaft clavicle fracture with ipsilateral AC joint injury.
Dr. Yogadeepan Dhakshinamurthi, Department of Orthopaedics, Dr. Muthus Hospital, Singanallur, Tamil Nadu, India. E-mail: yogadeepan5992@gmail.com
Introduction: Clavicle fractures and acromioclavicular (AC) joint disruptions are very common injuries. However, both injuries occurring simultaneously are very rare entities.
Case Report: In this article, we report a case of 21-year-old gentleman with a history of road traffic accident with a right mid-shaft clavicle fracture. We planned for the right clavicle plating. Intraoperatively incidentally, we found that the patient is having type 4 rockwood AC joint disruption with complete posterior displacement and gross instability. We repaired it after plating the clavicle using Ethibond with intraosseous sutures and augmented with trans acromion k wire. Later, k wire was removed, and the patient regained full range of motion shoulder after subsequent follow-up and physiotherapy.
Conclusion: Clavicle fractures with ipsilateral AC joint disruptions are very rare. Diagnosing the AC joint disruption and appropriate management is very essential to regain the shoulder function and outcome.
Keywords: Acromioclavicular joint, clavicle, Rockwood classification,Ethibond,K wire.
Clavicle fractures account for about 2.6% of total fractures [1]. Fractures of the clavicle and AC joint disruptions are very common. Both occur by mechanism of fall on an outstretched hand or fall on the lateral aspect of the shoulder [2]. However, both injuries in ipsilateral single bone are a very rare occurrence [3]. Usually, AC joint disruptions occur along with lateral end clavicle fractures but not commonly with middle or proximal third fractures [4]. Appropriate diagnosis of acromioclavicular (AC) joint dislocations in such cases and prompt management whether surgical or conservative is crucial in regaining the functional outcome of the patient. Surgical management for AC joint injuries includes a variety of techniques, such as suture anchor, endobutton, tight rope, k wire, dog bone, hook plate, and fiber wire.
We report a case of 21-year-old gentleman with a history of road traffic accident. He was diagnosed to have a right mid-shaft clavicle fracture (Fig. 1). Other injuries were ruled out.
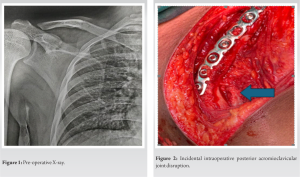
We have planned for the right clavicle plating. Under the interscalene block, the patient was positioned in the beach chair position. Under strict aseptic precautions, the clavicle fracture was opened; to our surprise, we found gross mobility of the distal fragment in the anteroposterior plane and complete detachment of the deltoid origin indicating type IV AC joint injury (Fig. 2). Clavicle shaft fracture was reduced and fixed using 9 hole 3.5 mm recon plate with 4 proximal and 4 distal cortical screws.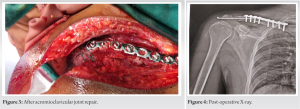
We decided to reduce and repair the AC joint. Intraosseous sutures were taken through the lateral end of the clavicle looping around the base of the coracoid along with the ruptured coracoclavicular ligaments. The ruptured muscle fibers of the deltoid origin were sutured back to the clavicle with intraosseous sutures. The AC joint was repaired using 5 Ethibond (Fig. 3). Joint was found to be stable. The repair was augmented by one 2 mm trans acromion k wire (Fig. 4). The patient postoperatively started on immediate passive shoulder flexion up to 90°. Suture removal was done at 2 weeks. He was on regular follow-up. K wire removal was done after 6 weeks. The patient regained full shoulder movements by the end of 8 weeks (Fig. 5).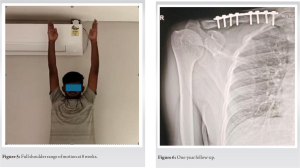
The patient now has 1-year follow-up (Fig. 6). He was doing all activities including heavy work, weightlifting, and playing. The patient has no pain or any functional disability.
The clavicle connects the arm and the trunk. Goss in 1993 described about superior shoulder suspensory complex concept where a soft tissue and bony ring on the superior shoulder maintain stability between the upper limb and axial skeleton [5]. AC joint is stabilized mainly by AC and coracoclavicular ligaments. Coracoclavicular ligaments comprise conoid and trapezoid ligaments. The incidence of mid-shaft clavicle fractures along with AC joint disruptions is very rare. Only a few cases have been reported in the literature [4, 6-11]. Marjoram and Chakrabarti study reveal that high-energy trauma results first in AC joint disruption followed by energy traveling along the clavicle axis inward causing mid-shaft clavicle fracture because of its inherent weakness [12]. Maruyama et al. [13] and Okano et al. [14] study revealed the “first rib pivot theory” for floating clavicle fracture. When the shoulder was struck with force, the scapula and clavicle move posteriorly together and inferiorly in relation to the trunk which results in AC joint disruption. The clavicle then stops moving downward due to contact with the first rib and tension from the deltoid muscle and hence clavicle fracture occurs with the first rib as pivot point. Prompt diagnosis of AC joint injury is very important. Otherwise, if it is missed and clavicle fracture is treated conservatively, it may lead to reduced loss of shoulder movements, pain, and disability, which was described in the Mohammed et al. study [15]. If any AC joint disruption is suspected along with clavicle fracture, X-ray modified Y view (Alexander view) or computed tomography (CT) scan can be taken to rule out the injury. In our case, we missed the AC joint injury because of type 4 injury which will not be seen in the usual anteroposterior X-ray view. In such a case, special X-ray views can be taken to rule out AC joint injuries [16]. CT scans in clavicle fractures are very useful in detecting associated lung injuries with hemothorax or pneumothorax which is a very common finding associated with direct impact injury on the shoulder. Ottomeyer et al. study showed that 96% of AC joint disruptions associated with clavicle fractures are type 2 or type 3 rockwood injuries [17]. In Van de Voort et al. review of case reports, 43% of AC joint injuries associated with clavicle fractures are type 4 injuries [18]. In this study, they found out that around 29 cases of clavicle fractures with AC joint disruption were reported in the literature and that three were managed conservatively and in two of the remaining 26 cases, only clavicle fracture was addressed and in all other 24 cases, AC joint also gets addressed along with clavicle fracture. Murray et al. study reveals that due to higher instability in view of the segmental nature of these injuries, there will be higher chances of non-union when opted for conservative management [19]. Fixation options for AC joints include a variety of options, such as endobutton, dog bone, suture anchor, k wires, hook plate, and fiber wire. Uittenbogaard et al. meta-analysis study in 2021 showed that there is no statistical difference in union rates while fixing AC joint disruption using different methods when done properly [20].
Clavicle fractures with ipsilateral AC joint disruptions although uncommon can occur following trauma. Prompt identification of AC joint disruption and appropriate management are necessary for ligament healing and good post-operative pain relief, full shoulder movements, and good long-term functional outcomes. Various fixation options are available for AC joints and almost all have good union rates.
AC joint injuries are most common along with lateral end clavicle fractures. Their occurrence with mid-shaft clavicle fractures is very rare and only a very few cases are reported in the literature. If any suspicion arises, necessary investigation needs to be done and if present, it should be managed appropriately to regain good shoulder movements and functional outcome.
References
- 1.Melenevsky Y, Yablon CM, Ramappa A, Hochman MG. Clavicle and acromioclavicular joint injuries: A review of imaging, treatment, and complications. Skeletal Radiol 2011; 40:831-42. [Google Scholar]
- 2.Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar]
- 3.Bakir MS, Carbon R, Ekkernkamp A, Schulz-Drost S. Monopolar and bipolar combination injuries of the clavicle: Retrospective incidence analysis and proposal of a new classification system. J Clin Med 2021;10:5674. [Google Scholar]
- 4.Psarakis S, Savvidou O, Voyaki S, Beltsios M, Kouvaras J. A rare injury of ipsilateral mid-third clavicle fracture with acromioclavicular joint dislocation. Hand (N Y) 2011;6:228-32. [Google Scholar]
- 5.Goss TP. Double disruptions of the superior shoulder suspensory complex. J Orthop Trauma 1993;7:99-106. [Google Scholar]
- 6.Lancourt JE. Acromioclavicular dislocation with adjacent clavicular fracture in a horseback rider. A case report. Am J Sports Med 1990;18:321-2. [Google Scholar]
- 7.Wurtz LD, Lyons FA, Rockwood CA Jr. Fracture of the middle third of the clavicle and dislocation of the acromioclavicular joint. A report of four cases. J Bone Joint Surg Am 1992;74:133-7. [Google Scholar]
- 8.Yeh PC, Miller SR, Cunningham JG, Sethi PM. Midshaft clavicle fracture and acromioclavicular dislocation: A case report of a rare injury. J Shoulder Elbow Surg 2009;18:e1-4. [Google Scholar]
- 9.Heinz WM, Misamore GW. Mid-shaft fracture of the clavicle with grade III acromioclavicular separation. J Shoulder Elbow Surg 1995;4:141-2. [Google Scholar]
- 10.Tidwell JE, Kennedy PM, McDonough EB. Concurrent treatment of a middle-third clavicle fracture and type IV acromioclavicular dislocation. Am J Orthop Belle Mead NJ 2014;43:E275-8. [Google Scholar]
- 11.Solooki S, Azad A. Simultaneous middle third clavicle fracture and type 3 acromioclavicular joint dislocation; a case report. Arch Bone Jt Surg 2014;2:69-71. [Google Scholar]
- 12.Marjoram TP, Chakrabarti A. Segmental clavicle fracture and acromio-clavicular joint disruption: An unusual case report. Shoulder Elbow 2015;7:187-9. [Google Scholar]
- 13.Maruyama K, Sugawara R, Sano S. “Similar case of panclavicular dislocation”. Katakansetsu 1984;8:147-50. [Google Scholar]
- 14.Okano I, Sawada T, Inagaki K. Bipolar dislocation of the clavicle: A report of two cases with different injury patterns and a literature review. Case Rep Orthop 2017;2017:2935308. [Google Scholar]
- 15.Mohammed KD, Stachiw D, Malone AA. Type IV acromioclavicular joint dislocation associated with a mid-shaft clavicle malunion. Int J Shoulder Surg 2016;10:37-40. [Google Scholar]
- 16.Gorbaty JD, Hsu JE, Gee AO. Classifications in brief: Rockwood classification of acromioclavicular joint separations. Clin Orthop Relat Res 2017;475:283-7. [Google Scholar]
- 17.Ottomeyer C, Taylor BC, Isaacson M, Martinez L, Ebaugh P, French BG. Midshaft clavicle fractures with associated ipsilateral acromioclavicular joint dislocations: Incidence and risk factors. Injury 2017;48:469-73. [Google Scholar]
- 18.Van de Voort JC, Van Doesburg PG, Leijnen M. Ipsilateral Rockwood type IV acromioclavicular joint dislocation and midshaft clavicle fracture: A case report and review of the literature Jan C. JSES Rev Rep Tech 2022;3:236-41. [Google Scholar]
- 19.Murray IR, Foster CJ, Eros A, Robinson CM. Risk factors for nonunion after nonoperative treatment of displaced midshaft fractures of the clavicle. J Bone Joint Surg Am 2013;95:1153-8. [Google Scholar]
- 20.Uittenbogaard SJ, Van Es LJ, Den Haan C, Van Deurzen DF, Van den Bekerom MP. Outcomes, union rate, and complications after operative and nonoperative treatments of neer type II distal clavicle fractures: A systematic review and meta-analysis of 2284 patients. Am J Sports Med Nov 2021;51(3):036354652110533. [Google Scholar]