Orthopedic surgeons should know the existence of posterior aspect fracture of the tibia as a rare complication specific to open wedge distal tuberosity osteotomy.
Dr. Hiroya Akase, Department of Orthopaedic Surgery, Oita University, 1-1 Idaigaoka Hazama-Machi, Yufu City, Oita, Japan. E-mail: k0741002ah@oita-u.ac.jp
Introduction: Open wedge distal tuberosity osteotomy (OWDTO) was the surgical treatment in which tibial tuberosity was attached proximal fragment to avoid an increase in patellofemoral joint pressure. The current paper reported a case of post-operative posterior aspect fracture of the tibia as a rare complication after OWDTO.
Case Report: A 52-year-old Asian man had been performing OWDTO for medial knee osteoarthritis. The patient was injured by the tibial posterior aspect fracture due to minor trauma 2 months after surgery. Bone union was completed by transient unloading and ultrasound therapy, but the anteroposterior screw remained in the bone due to screw breakage during removal.
Conclusion: Post-operative posterior aspect fracture of the tibia is a complication specific to OWDTO. It is difficult to detect the fracture on X-ray; therefore, the evaluation with computed tomography is recommended. It is possible that removal of the anteroposterior screw has become difficult in the event that this fracture occurs.
Keywords: Open wedge distal tuberosity osteotomy, complication, posterior aspect fracture of tibia, removal difficulty.
Knee osteotomy is a common surgery for young and active patients who have unicompartmental knee osteoarthritis. Open wedge high tibial osteotomy (OWHTO) [1] was the most popular osteotomy for medial unicompartmental knee osteoarthritis, but it was inevitable in OWHTO that patellofemoral joint pressure elevated due to distalization of tibial tuberosity [2]. Open wedge distal tuberosity osteotomy (OWDTO) was the surgical treatment reported by Gaasbeek et al. for the 1st time [3], tibial tuberosity was attached proximal fragment to avoid an increase of patellofemoral joint pressure. This technique was usually applied to patients who had patellofemoral degeneration in addition to medial knee osteoarthritis. Akiyama et al. [4] has reported modified OWDTO, cutting medial tuberosity in an arc shape to prevent medial protrusion of the distal side. We have adopted this method in operating OWDTO so far, but we experienced a case of post-operative posterior aspect fracture of the tibia. This fracture was uncommon and has not been reported before to our knowledge. This is the first report about this rare complication specific to OWDTO.
A 52-years-old Asian man had right knee pain for 3 years. There was no history of previous trauma. There were diabetes mellitus as a history and obese (height 1.75 m weight 93.0 kg body mass index 30.4 kg/m2). Before refer to our hospital, the patient had undergone an arthroscopic medial meniscectomy in another hospital, but the symptoms had not improved. The pain was localized medial joint line, but there was also mild patellofemoral joint tenderness. Joint instability tests, such as the Lachman test and posterior drawer test, were negative. In a radiographic examination, the medial femorotibial joint space was narrowed obviously, and we were diagnosed with Kellgren-Lawrence grade 2 knee osteoarthritis. For various measurement parameters, hip-knee-ankle angle was 3° varus, medial proximal tibial angle (MPTA) was 83°, mechanical lateral distal femoral angle was 86°, posterior tibial slope (PTS) was 12°, weight-bearing line ratio (WBL ratio) was 34.7% (Fig. 1). In MRI, there weren’t any other finding causing symptom other than osteoarthritis, such as ligament and lateral meniscus injury. He was a cleaning staff, which required high activity. Hence, we planned OWDTO with fewer activity restrictions.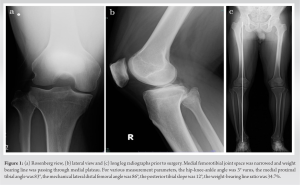
The correction angle was measured as 9° with the Miniaci method [5] so that the WBL ratio was 62.5%. The osteotomy site was fixed with a locking plate (Olympus Terumo Biomaterials, Tokyo, Japan) and cannulated cancellous screw (HOLLYX, Shizuoka, Japan) was inserted at the tuberosity anteroposteriorly for the purpose of stabilizing the sagittal plane. Post-operative X-ray showed Fig. 2.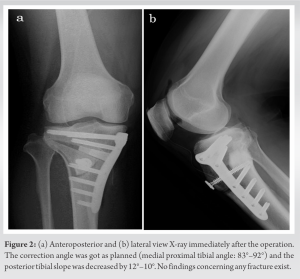
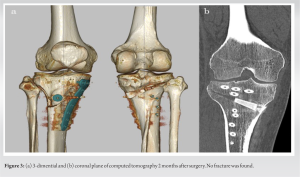
MPTA increased 83°–92°, planned correction angle was got and PTS was decreased from 12° to 10°. Two weeks later, we evaluated computed tomography, any fracture including lateral hinge fracture did not exist (Fig. 3).
Postoperatively, Range of motion and quadriceps strengthening exercise was started on the following day. The patient was allowed half partial weight-bearing a week later, full weight-bearing was permitted from 6 weeks later as much as the pain wasn’t terrible.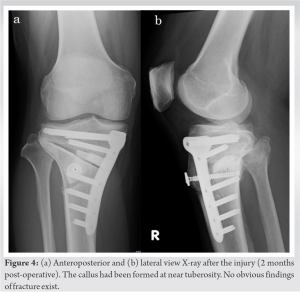
The patient spent performing rehabilitation and acquired a stable gait 2 months later. On discharge day, he injured an operative limb by stepping on the ground when he got out of the car. His knee pain got worse than ever, however, we weren’t able to detect any fracture sign on X-ray (Fig. 4). 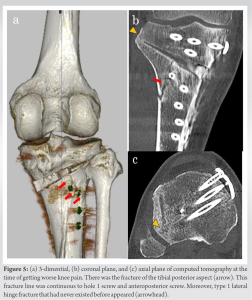
Because his symptoms were severe to be considered a sprain, we evaluated on computer tomography and detected the fracture on the tibial posterior aspect of distal fragment. The fracture line penetrated between the screws and occurred only on the posterior surface, which was different from a typical axial pressure injury such as a tibial plateau fracture. Moreover, a lateral hinge fracture that had not ever been found appeared (Fig. 5). We instructed him to unload with a cane for a month and began low-intensity pulsed ultrasound. After that, healing was delayed, but the osteotomy gap was gradually filled. Bone union was completed in post-operative 20 months. The implant removal was performed 22 months after surgery due to the irritation of the locking plate. However, the cannulated cancellous screw was broken in the junction of the head and thread during removal, the part of the thread remained in bone. Although coronal alignment has not changed from primary surgery to implant removal, PTS increased from 10° to 13° in recent X-ray compared to the time of surgery (Fig. 6). His knee pain was relieved; the Lysholm score was improved from 48 to 78 points in post-operative 2 years.
We instructed him to unload with a cane for a month and began low-intensity pulsed ultrasound. After that, healing was delayed, but the osteotomy gap was gradually filled. Bone union was completed in post-operative 20 months. The implant removal was performed 22 months after surgery due to the irritation of the locking plate. However, the cannulated cancellous screw was broken in the junction of the head and thread during removal, the part of the thread remained in bone. Although coronal alignment has not changed from primary surgery to implant removal, PTS increased from 10° to 13° in recent X-ray compared to the time of surgery (Fig. 6). His knee pain was relieved; the Lysholm score was improved from 48 to 78 points in post-operative 2 years.
Overall complication rates were 37–55% after OWHTO in a previous study [6]. Among those, lateral hinge fracture was the most common complication in OWHTO, reported 19.8–25.0% [6,7]. Regarding OWDTO, tuberosity fracture was characteristic, the incidence had been reported as 11.5% [7,8]. However, there were few reports on other fractures except these fractures, and no report showing posterior aspect fracture of the tibia after OWDTO existed. The direct cause of this fracture was extreme axial load in the period that bone healing was incomplete. In addition, it was possible as another cause that the hole 1 screw of the tris plate and the cannulated cancellous screw were in close proximity (Fig. 5). Actually, this fracture continued these screws. Furthermore, a lateral hinge fracture was also present when this fracture happened. The lateral hinge fracture was classified as type 1 in the Takeuchi classification [7], a previous study described this type didn’t decline stability of the osteotomy site [9]. On the other hand, Lee showed that the PTS was increased by almost 2° in the posterior subtype, fracture line pierced through the posterior to the midline, compared to the anterior subtype among type 1 lateral hinge fracture [10]. This result indicated when type 1 lateral hinge fracture occurred posteriorly, the posterior part of the osteotomy site suffered additional compressive force. In fact, PTS increased compared to an early post-operative period at the past follow-up in this case, the fracture might have been a trigger in the posterior aspect fracture. At the time of removal, the cannulated cancellous screw was broken. The incident was caused to the sclerotic bone surrounding the screw tip which had formed during healing in addition to a long period of time until removal (Fig. 7). This bone was usually formed in the bone fusion process, so particular attention should be paid to removal difficulty when posterior aspect fracture of the tibia was happened.
Post-operative posterior aspect fracture of the tibia is an uncommon complication after OWDTO. This complication is specific to OWDTO, and it’s difficult to detect the fracture on X-ray. If the knee pain gets worse triggered by some kind of trauma post-operatively, evaluation with computed tomography is recommended to avoid missing this fracture. It could be a factor that the hole 1 screw and the anteroposterior screw are nearby, we need caution about the plate position and the direction of the anteroposterior screw. Moreover, it is possible that removal of the anteroposterior screw has become difficult in the event that this fracture occurs.
Post-operative posterior aspect fracture of the tibia is a specific complication after OWDTO. If the sudden onset of pain happens postoperatively, performing computed tomography is recommended with the possibility of this fracture in mind.
References
- 1.Staubli AE, Simoni CD, Babst R, Lobenhoffer P. Tomofix: A new LCP-concept for open wedge osteotomy of the medial proximal tibia-early resulrs in 92 cases. Injury 2003;34:55-62. [Google Scholar]
- 2.Yang JS, Fulkerson JP, Obopilwe E, Voss A, Divenere J, Mazzocca AD, et al. Patellofemoral contact pressures after patellar distalization: A biomechanical study. Arthroscopy 2017;33:2038-4. [Google Scholar]
- 3.Gaasbeek RD, Sonneveld H, Heerwaarden RJ, Jacobs WC, Wymenga AB. Distal tuberosity osteotomy in open wedge high tibial osteotomy can prevent patella infera: A new technique. Knee 2004;11:457-61. [Google Scholar]
- 4.Akiyama T, Osano K, Mizu-Uchi H, Nakamura N, Okazaki K, Nakayama H, et al. Distal tibial tuberosity arc osteotomy in open-wedge proximal tibial osteotomy to prevent patella infra. Arthrosc Tech 2019;8:655-62. [Google Scholar]
- 5.Miniaci A, Ballmer FT, Ballmer PM, Jakob RP. Proximal tibial osteotomy. A new fixation device. Clin Orthop Relat Res 1989;246:250-9. [Google Scholar]
- 6.Martin R, Birmingham TB, Willits K, Litchfield R, Lebel ME, Giffin R. Adverse event rates and classifications in medial opening wedge high tibial osteotomy. Am J Sports Med 2014;42:1128-6. [Google Scholar]
- 7.Takeuchi R, Ishikawa H, Kumagai K, Yamaguchi Y, Chiba N, Akamatsu Y, et al. Fractures around the lateral cortical hinge after a medial opening-wedge high tibial osteotomy: A new classification of lateral hinge fracture. Arthroscopy 2012;28:85-94. [Google Scholar]
- 8.Ogawa H, Matsumoto K, Yoshioka H, Sengoku M, Akiyama H. Fracture of the tibial tubercle does not affect clinical outcomes in medial opening wedge high tibial osteotomy with distal tibial tubercle osteotomy. Arch Orthop Trauma Surg 2022;142:607-13. [Google Scholar]
- 9.Kang KT, Koh YG, Lee JA, Lee JJ, Kwon SK. Biomechanical effect of a lateral hinge fracture for a medial opening wedge high tibial osteotomy: Finite element study. J Orthop Surg Res 2020;15:63. [Google Scholar]
- 10.Lee SS, Nha KW, Lee DH. Posterior cortical breakage leads to posterior tibial slope change in lateral hinge fracture following opening wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 2019;27:698-706. [Google Scholar]