
Individuals who present with complaints of knee pain and restricted deep flexion, mucoid degeneration of the ACL, or femur ganglion cyst should be given careful consideration.
Dr. Syed Kareemulla, Department of Orthopaedics and Traumatology, Amulya Nursing Home, Narasaraopet, Andhra Pradesh, India. E-mail: sdkarim1926@@gmail.com
Abstract
Introduction: A ganglion cyst is just an accumulation of gelatinous fluid in thick covering that develops from the capsules around tendons or joints . The cause is unknown; however, several suggestions have been put forth, including ectopic tissue development, synovial herniation, and trauma . The clinical symptoms differ based on the location. Management techniques such as non-operative, computed tomography-guided aspiration, open debridement, arthroscopic debridement, and decompression are advised.
Case Report: Here, we report a 32-year-old man who had no history of severe trauma but had been complaining of knee flexion pain for the previous 3 years. There is no clinical laxity, and no additional injuries were observed. The patient had a magnetic resonance imaging (MRI) and an X-ray conducted. X-ray appears normal. The femur foot print location has a big cystic lesion seen on the MRI, located behind the ACL. No other anomalies are found.
Conclusion: Femoral ganglion cysts are frequently missed but can be diagnosed with the use of a clinical examination and a link between the clinical findings and MRI. The pain is reduced with arthroscopic cyst decompression.
Keywords: Femur ganglion cyst, arthroscopic cyst, decompression.
The first intra-articular cyst within anterior cruciate ligament (ACL) was described in 1924 by Caan [1]. Numerous etiologies have been hypothesized for ganglion cysts connective tissue mucinous degeneration, ectopic tissue development, and trauma [2-4]. The most frequent location is the wrist, while the most common location in the knee is the anterior cruciate ligament (ACL), followed by the meniscus and posterior cruciate ligament [5]. According to published research, ganglia associated with the ACL are present in 0.12–0.44% of cases of magnetic resonance imaging (MRI) [6,7]. Ganglion cysts do not happen very often. The ACL is frequently impacted. ACL, posterior cruciate ligament (PCL), and meniscus are the only additional structures where ganglion cysts are frequently found. The infrapatellar fat pad, medial plica, and popliteus are the three locations where they are the least common [8]. Either one or more of them exist. Often unilateral, reports of bilateral presentations are also occasionally made. Meniscal tears have been linked to ganglion cysts on occasion. The ACL ganglion cysts are rarely symptomatic. They should be confirmed with an MRI to rule out other pathologies. Then, depending on their location they are managed either by computed tomography (CT)-guided aspiration for cysts behind PCL or arthroscopic debridement and excision to prevent recurrence.
A 32-year-old male patient arrived complaining of soreness across the back of his right knee that had persisted for 2 years without any prior trauma history.
Clinical findings
Before surgery, clinical testing was done, and there were no indications of instability. There is deep flexion pain, but there is no ultimate restriction to extension or indications of instability.
Diagnostic assessment
The patient was instructed to have X-rays and a knee MRI to be further evaluated. X-rays show no abnormalities, and when an MRI of the knee was performed, a cystic lesion was seen in the t2 saggital portion of the knee, encircling the posterior part of the ACL at the femur footprint (Fig. 1).
Surgical technique
Evaluation portals used
Portal A – Standard arthroscopic anterolateral (AL) portal which is 1 cm inferior and lateral to the inferior pole of patella
Portal B – Standard anteromedial (AM) portal which is determined using a spinal needle (Fig. 2).
Surgical technique
The patient is placed supine under spinal anesthesia, and an 11-bladed conventional arthroscopic AL portal is created. After a diagnostic arthroscopy, a ganglion cyst located behind the ACL (Fig. 3) is discovered; the menisci and cartilage are unaffected.
Anteromedial portal placement, shaving, and debridement of the Hoffa fat pad are performed with the aid of a spinal needle. Using a radiofrequency probe and portal switching, the ganglion cyst behind the ACL is excised.
Fig. 4 shows that there are no indications of instability following decompression – Bandage application and wound closure.
Post-operative rehabilitation
Weight-bearing is allowed on day 1. Ankle pumps and gluteal strengthening exercises are started. Quadriceps strengthening is started, and knee core strengthening exercises have been done. Was the tissue/fluid sent for CS/histopathology? No biopsy or culture has been sent for study of the tissue or fluid. What was the last follow-up? And outcome? When the ACL laxity was eventually examined, no laxity was observed. The patient experienced no pain during their 6-month follow-up.
ACL ganglion cysts are quite uncommon. Numerous theories have been put out concerning the etiology. The majority of ganglion cysts show no symptoms. It is crucial to do a thorough clinical evaluation, which should be supported by MRI imaging. They range in size from 5 to 30 mm and have a variety of forms, including fusiform spindle and oval. Our measured cyst measured 22 by 12 mm, directly behind the ACL. Since ganglion cysts are circumscribed masses without locules, MRI is an adequate tool for distinguishing them from other disorders, such as pigmented villonodular cysts and mucoid degeneration. Krudwig et al. documented 85 instances of intra-articular ganglion cysts, of which 9 were symptomatic and the remaining 76 were asymptomatic. All 9 patients had no prior history of trauma. There are several approaches to treating intra-articular ganglions. They were given conservative treatment if they were incidental observations and asymptomatic. Surgery is necessary for the symptomatic cysts. Arthroscopic debridement, excision, and needle aspiration were the methods. Nokes et al. used CT guidance to aspirate PCL ganglion cysts to avoid damaging neurovascular tissues [10]. Arthroscopy offers more accurate and straightforward visualization. The portals used varied according to the location of the cyst. The cyst that is present at the tibia footprint of the ACL and intrasubstance of the ACL can be adequately treated by the usual AM and AL portals. For thorough debridement and excision that prevents recurrence, cysts that were not receptive to am and al portals, such as cysts behind PCL, require additional portals. We should be equipped with instrumentation for reconstruction intra-operatively if there is a need. We performed arthroscopy using AM and AL portals, which are sufficient for adequate decompression and debridement.
Patients who have internal knee derangement, complain of pain over the knee, and have a terminal loss of range of motion should be thoroughly clinically assessed. Additional testing, such as MRIs, may be necessary. MRI suffices for the confirmation. For ganglion cysts, arthroscopic debridement and excision is the usual course of treatment to avoid recurrence.
It is quite uncommon for an ACL ganglion cyst to present. The presentation of clinical symptoms varies in the region, presenting as discomfort and impaired deep flexion or extension. With MRI, they ought to be verified.
References
- 1.Caan P. Cyst formation (ganglion) in an anterior cruciate ligament of the knee. Deutsch Z Chir 1924;186:403-8. [Google Scholar | PubMed]
- 2.McIntyre J, Moellelen S, Tirman T. Mucoid degeneration of the anterior cruciate ligament mistaken for ligamentous tears. Skeletal Radiol 2001;30:312-5. [Google Scholar | PubMed]
- 3.Fealy S, Kenter K, Dines JS, Warren RF. Mucoid degeneration of the anterior cruciate ligament. Arthroscopy 2001;17:37-9. [Google Scholar | PubMed]
- 4.Maffulli N, Binfield PM, King JB. Isolated ganglions of the anterior cruciate ligament. Med Sci Sports Exerc 1993;25:550-3. [Google Scholar | PubMed]
- 5.Vaishya R, Esin Issa A, Agarwal AK, Vijay V. Anterior cruciate ligament ganglion cyst and mucoid degeneration: A review. Cureus 2017;9:e1682. [Google Scholar | PubMed]
- 6.Do-Dai DD, Youngberg RA, Lanchbury FD, Pitcher JD Jr., Garver TH. Intraligamentous ganglion cysts of the anterior cruciate ligament: MR findings with clinical and arthroscopic correlations. J Comput Assist Tomogr 1996;20:80-4. [Google Scholar | PubMed]
- 7.Huang GS, Lee CH, Chan WP, Taylor JA, Hsueh CJ, Juan CJ, et al. Ganglion cysts of the cruciate ligaments. Acta Radiol 2002;43:419-24. [Google Scholar | PubMed]
- 8.Kang CN, Kim DW, Kim DJ, Kim SJ. Intra-articular ganglion cysts of the knee. Arthroscopy 1999;15:373-8. [Google Scholar | PubMed]
- 9.Krudwig WK, Schulte KK, Heinemann C. Intra-articular ganglion cysts of the knee joint: A report of 85 cases and review of the literature. Knee Surg Sports Traumatol Arthrosc 2004;12:123-9. [Google Scholar | PubMed]
- 10.Nokes SR, Koonce TW, Montanez J. Ganglion cysts of the cruciate ligaments of the knee: Recognition on MR images and CT-guided aspiration. Am J Roentgenol 1994;162:1503. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Spinal Stenosis in Achondroplasia – A Case Report and Review of the Literature
November 1, 2025 Spinal Stenosis in Achondroplasia – A Case Report and Review of the Literature July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture
July 1, 2025 Case Report – Surgical Management and Neurological Recovery in an 18-Year-Old Male with C4-C5 Cervical Spine Fracture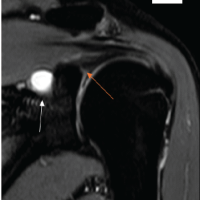 March 1, 2025 Glenoid Paralabral Cysts Causing Shoulder Pain and Isolated Infraspinatus Weakness: Early Arthroscopic Decompression and Labral Repair Leads to Complete Recovery: A Case Series
March 1, 2025 Glenoid Paralabral Cysts Causing Shoulder Pain and Isolated Infraspinatus Weakness: Early Arthroscopic Decompression and Labral Repair Leads to Complete Recovery: A Case Series August 6, 2024 Core Decompression with Bone Marrow Aspirate Concentrate Implantation in Osteonecrosis of the Femoral Head with a Minimum of 2-year Follow-up – A Pilot Study
August 6, 2024 Core Decompression with Bone Marrow Aspirate Concentrate Implantation in Osteonecrosis of the Femoral Head with a Minimum of 2-year Follow-up – A Pilot Study