
Unusual presentation of fractures should raise alarm and complete medical evaluation should be done rather than just fixation of the fracture so that recurrence is prevented and proper treatment of the patient is done.
Dr. Mansoor Malnas, Postgraduate Student, Department of Orthopaedics, Bombay Hospital, New Marine Lines, Mumbai, Maharashtra, India. E-mail: malnasmansoor@gmail.com
Abstract
Introduction: An atypical bone fracture is a complete or partial discontinuity of bone which occurs without sufficient trauma. Autoimmune polyglandular syndromes are complex conditions characterized by the simultaneous presence of at least two autoimmune-mediated endocrinopathies. These syndromes exhibit considerable heterogeneity in their manifestations and typically unfold sequentially, with a significant time gap between the onset of the initial and subsequent glandular autoimmune diseases. In this article, we report a case of bilateral subtrochanteric atypical fractures in a patient with autoimmune polyglandular syndrome. This case scenario has not been reported in the literature so far to the best of our knowledge.
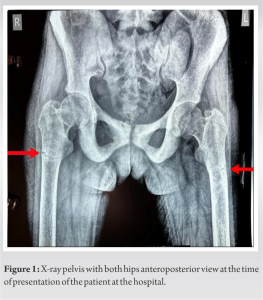
Case Report: A 37-year-old female patient presented at a tertiary care center in a metropolitan city with complaints of pain in both hips and the upper thigh. The patient faced difficulty walking and was unable to do so due to severe pain. Notably, there was no history of a fall or trauma. A radiographic examination revealed bilateral subtrochanteric atypical fractures. Upon further investigation, the patient was also found to be having hypothyroidism, hypoparathyroidism, pancytopenia, and an autoimmune disorder. The patient received a diagnosis of Autoimmune polyglandular syndrome with bilateral subtrochanteric atypical fractures. Treatment involved a comprehensive approach, including thyroxine for hypothyroidism, low-dose steroids, immunosuppressive agents, calcium supplementation, parathyroid hormone, and transfusion of blood and blood products. Due to the fractures being extra-articular, incomplete, and undisplaced, a conservative management approach was adopted.
Conclusion: The occurrence of atypical and pathological fractures, particularly when bilateral or recurrent, necessitates a comprehensive evaluation to determine the root cause. It is imperative to address the underlying etiology thoroughly in every patient. Neglecting to do so may lead to a recurrence or insufficient resolution of the pathology. In instances where two or more endocrine organs are involved, consideration should be given to autoimmune polyglandular syndrome as a potential diagnosis.
Keywords: Atypical fracture, bilateral subtrochanteric fracture, autoimmune polyglandular syndrome.
Atypical femoral fractures are stress fractures that typically begin in the lateral shaft of the femur. They can occur with minimal or no trauma and exhibit distinct radiographic characteristics. These fractures may manifest in individuals both with and without a history of taking antiresorptive osteoporosis medications. The American Society for Bone and Mineral Research outlines the case definition for atypical femur fracture as follows [1]. The fracture must be situated along the femoral diaphysis, spanning from just below the lesser trochanter to slightly above the supracondylar flare. Moreover, a minimum of four out of five major features must be identifiable. While none of the minor features are obligatory, they have occasionally been observed in association with these fractures.
Major features
- The fracture occurs with minimal or no discernible trauma, resembling a fall from standing height or less
- Its trajectory typically originates at the lateral cortex and maintains a predominantly transverse orientation, although it may transition to an oblique alignment as it traverses medially across the femur
- Complete fractures extend through both cortices and may be accompanied by a medial spike, whereas incomplete fractures involve solely the lateral cortex
- The fracture is characterized by non-comminuted or minimally comminuted patterns
- Localized thickening of the lateral cortex at the fracture site, often termed “beaking” or “flaring,” is observable.
Minor features
- Generalized augmentation in cortical thickness along the femoral diaphyses
- Presence of unilateral or bilateral prodromal symptoms, such as dull or aching pain in the groin or thigh
- Occurrence of bilateral incomplete or complete femoral diaphysis fractures
- Delayed progression of fracture healing.
The autoimmune polyglandular syndromes are clusters of endocrine abnormalities that occur in discreet patterns in subjects with immune dysregulation and that permit treatment and anticipation of associated systemic or other hormonal deficiencies [2]. They are complex conditions characterized by the simultaneous presence of at least two autoimmune-mediated endocrinopathies. These syndromes exhibit considerable heterogeneity in their manifestations and typically unfold sequentially, with a significant time gap between the onset of the initial and subsequent glandular autoimmune diseases. In this article, we report a case of bilateral subtrochanteric atypical fractures in a patient with autoimmune polyglandular syndrome. This case scenario has not been reported in the literature so far to the best of our knowledge.
A 37-year-old female from a rural village sought medical attention at a tertiary care center in a metropolitan city. She presented with pain in both upper thighs and hips, along with discomfort while standing and difficulty walking. There was no history of falls or trauma. The patient was previously asymptomatic until 2–3 months ago when she began experiencing pain in her right leg, which was insidious in onset and gradually worsened. One month later, similar symptoms developed in her left leg. A radiographic examination confirmed bilateral subtrochanteric atypical fractures (Fig. 1). Further history revealed that the patient had previously undergone surgery on her left femur 3 years ago for intramedullary nailing due to similar complaints, and implant removal was performed 1 year ago. Bilateral and/or recurrent atypical fractures are uncommon and raise suspicion of an underlying systemic condition. The patient underwent investigations, revealing hypothyroidism, hypoparathyroidism, pancytopenia, and an autoimmune disorder. Consultations were sought from endocrinology, hematology, and rheumatology specialists.
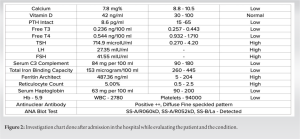
Magnetic resonance imaging (MRI) of both hips showed diffuse abnormal altered marrow signals affecting the pelvic bones and lumbosacral spine, suggestive of generalized osteosclerosis. In addition, abnormal intramedullary signals were observed in the bilateral femoral metaphysis and diaphysis, indicating a possible underlying diffuse bone marrow or hematopoietic disorder, or metabolic bone disorder. Incomplete stress or partial pathological fractures involving the outer cortex of both femurs in the meta-diaphysis region were noted. Red marrow signals were also present in the bilateral femoral neck and proximal metaphysis. Thyroid ultrasound revealed a small-sized thyroid gland with diffusely heterogeneous echotexture, indicative of chronic thyroiditis. Complete blood evaluation and investigations were conducted, with positive findings as described in Fig. 2.
The comprehensive work-up of the patient led to the diagnosis of autoimmune polyglandular syndrome. Treatment was initiated accordingly:
- Hypothyroidism: Managed with thyroxine supplementation
- Hypoparathyroidism: Addressed with calcium and parathyroid hormone (PTH) supplementation
- Pancytopenia: Required transfusion of blood and blood products to address the low blood cell counts
- Autoimmune disorder: Treated with immunosuppressive drugs and low-dose steroids to alleviate inflammatory processes throughout the body.
As for the fractures, they were managed conservatively due to being incomplete, undisplaced, and extra-articular. This approach aimed to allow natural healing without the need for surgical intervention.
Atypical femoral fractures are stress fractures that typically begin in the lateral shaft of the femur. They can occur with minimal or no trauma and exhibit distinct radiographic characteristics. These fractures may manifest in individuals both with and without a history of taking antiresorptive osteoporosis medications. The characteristic features of atypical femoral fractures, including the presence of “the dreaded black line,” have been observed in patients. This comparison of different features eventually led to the definition provided by the American Society for Bone and Mineral Research in 2010. This definition is particularly useful in cases of complete fractures, but it is also crucial to diagnose and treat impending fractures before they progress to completion. Identifying impending fractures can be challenging and requires a high index of suspicion, especially in patients with a history of osteoporosis, particularly if they are currently or have recently been treated with bisphosphonates or other prophylactic medications and are experiencing thigh or groin pain, even if the treatment duration was brief. When there is suspicion of incomplete atypical femoral fractures, careful radiographic examination for features suggestive of impending fractures on hip and pelvic radiographs is necessary. In cases of complete fracture, the contralateral side should also be radiographed and meticulously inspected for transverse fracture lines in the lateral cortex, beaking, and other characteristic signs of atypical femoral fracture, as bilateral involvement occurs in 40% or more of cases [3]. The sensitivity and specificity of these signs are generally high, especially for transverse fracture lines, lack of comminution, and localized periosteal or endosteal thickening of the lateral cortex [4]. If radiographs of the contralateral side appear normal but clinical suspicion persists, computed tomography (CT) should be considered fracture lines not visible on radiographs may be detected. Studies have shown that patients who subsequently experience atypical femoral fractures have thicker lateral cortex in the subtrochanteric region of the femur on CT before the fracture event compared to bisphosphonate users who did not sustain a femoral fracture and bisphosphonate-naïve patients [5]. Therefore, CT may be used for the early detection of atypical femoral fractures. In addition, MRI can reveal periosteal and endosteal edema, which may also indicate an impending fracture and can be useful in the conservative follow-up of impending fractures. While atypical femur fractures have been primarily associated with the use of bisphosphonates, they can also occur in patients with no exposure to these drugs. Other pharmacological treatments that decrease bone turnover have similar consequences regarding the risk of these fractures. In addition, systemic diseases such as non-Hodgkin’s lymphoma, autoimmune polyglandular syndrome, and bone diseases such as hypophosphatasia, pycnodysostosis, and osteopetrosis, as well as Vitamin D deficiency and rheumatoid arthritis, can also lead to similar structural bone changes predisposing individuals to atypical femur fractures [6]. These conditions directly affect bone structure in a manner akin to the effects of bisphosphonates. In a Korean multicenter study, bone mineral density, prodromal symptoms, and medication history for osteoporosis were retrospectively analyzed in 76 cases of atypical femoral fracture [7]. Twenty-two patients (28.9%) experienced prodromal symptoms, whereas 43 (56.5%) exhibited delayed fracture union, and bilateral femoral fractures developed in 23 cases (30.2%). Apart from prolonged and continuous use of bisphosphonates, long-term glucocorticoid use, and a higher body mass index were identified as risk factors predisposing individuals to atypical femur fractures [8]. Furthermore, biomechanical factors such as anterolateral femoral bowing and loss of thigh muscle were found to influence the occurrence of these fractures [9]. The autoimmune polyglandular syndromes are clusters of endocrine abnormalities that occur in discreet patterns in subjects with immune dysregulation and that permit treatment and anticipation of associated systemic or other hormonal deficiencies. They are complex conditions characterized by the simultaneous presence of at least two autoimmune-mediated endocrinopathies. These syndromes exhibit considerable heterogeneity in their manifestations and typically unfold sequentially, with a significant time gap between the onset of the initial and subsequent glandular autoimmune diseases. The underlying autoimmune reaction in autoimmune polyglandular syndromes typically involves the production of autoantibodies against endocrine tissues, cell-mediated autoimmunity, or a combination of both mechanisms. This immune response results in inflammation, lymphocytic infiltration, and partial or complete destruction of the affected glands. It is common for more than one endocrine gland to be involved, although clinical manifestations may not always occur simultaneously. The clinical presentation of patients with autoimmune polyglandular syndromes reflects the cumulative effects of individual endocrine deficiencies and associated non-endocrine disorders. Importantly, these deficiencies may not manifest simultaneously and could require several years to become evident. In some cases, there may not be a specific sequence in which the deficiencies appear. Due to the variability and complexity of these syndromes, patients may exhibit a wide range of symptoms and signs related to the affected endocrine glands. These manifestations can include hormonal imbalances, such as hypothyroidism, hypoparathyroidism, adrenal insufficiency, and diabetes mellitus, among others. In addition, patients may experience symptoms related to non-endocrine disorders, which could result from autoimmune reactions or other systemic effects of the underlying condition. In addition to affecting endocrine tissues, the autoimmune reaction and associated dysfunction of the immune system can also lead to damage in non-endocrine tissues. This broader immune dysregulation can contribute to a range of systemic manifestations beyond the endocrine system. The diagnosis of polyglandular deficiency syndromes is typically suggested based on clinical presentation and confirmed by detecting deficient hormone levels through laboratory testing. It is important to differentiate these syndromes from other causes of multiple endocrine deficiencies, such as hypothalamic-pituitary dysfunction or coincidental endocrine dysfunction due to separate causes. In general, management of autoimmune polyendocrine syndromes includes hormone-replacement therapy as needed and treatment of complications [10]. For patients diagnosed with atypical femur fractures, whether as a stress reaction, stress fracture, incomplete or complete subtrochanteric, or femoral shaft fracture, discontinuation of bisphosphonates or other potent antiresorptive agents is recommended. It is essential to assess the patient’s dietary calcium and Vitamin D status and provide adequate supplementation as needed. In cases of atypical femur fractures, simple fixation alone may not suffice, and it is crucial to optimize the patient’s bone metabolic profile while discontinuing any potential influencing factors. Failure to do so may impede healing and even lead to treatment failure [11]. However, the optimal duration of bisphosphonate discontinuation remains uncertain, and whether these agents can be resumed after a “drug holiday” of 3–5 years requires further investigation [12]. Teriparatide, a recombinant form of PTH, has been suggested as a potential adjunctive treatment for atypical femur fractures, given its ability to enhance bone healing, particularly in cases of delayed healing or non-union. However, clinical evidence supporting the use of teriparatide in atypical femur fracture treatment is limited [13], and its routine use cannot be recommended until further research establishes its efficacy and safety specifically in this context. Other treatment modalities, such as low-intensity pulsed ultrasound [14] and bone marrow aspirate concentrate [15], have been investigated in small retrospective series and case–control studies for their potential benefits in atypical femur fracture management. However, the evidence supporting their effectiveness remains insufficient to draw definitive conclusions, and further research is warranted to ascertain their role in atypical femur fracture treatment.
The presented case highlights the complexity and challenges associated with atypical femur fractures, particularly in the context of impending fractures and delayed healing or non-union. Through a comprehensive review of the literature, several key findings have emerged, shedding light on the predictors of complete fractures, factors influencing healing outcomes, and the intricacies of surgical management. The case underscores the importance of identifying impending fractures in patients with a history of osteoporosis or antiresorptive medication use, as early intervention can mitigate the risk of progression to complete fractures. Furthermore, it emphasizes the need for meticulous surgical techniques, including restoration of the anatomical neck-shaft angle, to optimize healing outcomes and minimize complications. This case report holds significance across various clinical specialties, including orthopedics, endocrinology, hematology, and rheumatology, as it contributes to our understanding of the pathogenesis, diagnosis, and management of autoimmune polyglandular syndrome. By elucidating the factors associated with delayed healing and non-union, it provides valuable insights for clinicians in optimizing treatment strategies and improving patient outcomes. Moreover, this report underscores the importance of ongoing research and clinical vigilance in addressing the complexities of autoimmune polyglandular syndrome and atypical femoral fractures, particularly in light of the rising prevalence of osteoporosis and the widespread use of antiresorptive medications. By advancing our knowledge of disease etiology, surgical techniques, and pathology, this case report has the potential to significantly impact clinical practice and enhance patient care in a broader context across medicine.
The occurrence of atypical and pathological fractures, particularly when bilateral or recurrent, necessitates a comprehensive evaluation to determine the root cause. It is imperative to address the underlying etiology thoroughly in every patient. Neglecting to do so may lead to a recurrence or insufficient resolution of the pathology. In instances where two or more endocrine organs are involved, consideration should be given to autoimmune polyglandular syndrome as a potential diagnosis.
References
- 1.Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, et al. Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American Society for bone and mineral research. J Bone Miner Res 2014;29:1-23. [Google Scholar | PubMed]
- 2.Sperling MA, Angelousi A, Yau M. Autoimmune polyglandular syndromes. In: Feingold KR, Anawalt B, Blackman MR, Boyce A, Chrousos G, Corpas E, et al., editors. Endotext. South Dartmouth, MA: MDText.com, Inc.; 2000. [Google Scholar | PubMed]
- 3.Schilcher J, Aspenberg P. Incidence of stress fractures of the femoral shaft in women treated with bisphosphonate. Acta Orthop 2009;80:413-5. [Google Scholar | PubMed]
- 4.Adams Al, Xue F, Chantra JQ, Dell RM, Ott SM, Silverman S, et al. Sensitivity and specificity of radiographic characteristics in atypical femoral fractures. Osteoporos Int 2017;28:413-7. [Google Scholar | PubMed]
- 5.Lee SH, Lee YH, Suh JS. Lateral cortical thickening and bone heterogeneity of the subtrochanteric femur measured with quantitative CT as indicators for early detection of atypical femoral fractures in long-term bisphosphonate users. AJR Am J Roentgenol 2017;209:867-73. [Google Scholar | PubMed]
- 6.Saviola G, Prometti P, Ferrari PR, Dalle Carbonare LG. Atypical femoral fracture as first sign of non-hodgkin lymphoma-case report with a brief review of the literature. Clin Ter 2016;167:188-90. [Google Scholar | PubMed]
- 7.Kang Js, Won YY, Kim JO, Min BW, Lee KH, Park KK, et al. Atypical femoral fractures after anti-osteoporotic medication: A Korean multicenter study. Int Orthop 2014;38:1247-53. [Google Scholar | PubMed]
- 8.Koh JH, Myong JP, Yoo J, Lim YW, Lee J, Kwok SK, et al. Predisposing factors associated with atypical femur fracture among postmenopausal Korean women receiving bisphosphonate therapy: 8 years’ experience in a single center. Osteoporos Int 2017;28:3251-9. [Google Scholar | PubMed]
- 9.Shin WC, Moon NH, Jang JH, Park KY, Suh KT. Anterolateral femoral bowing and loss of thigh muscle are associated with occurrence of atypical femoral fracture: Effect of failed tension band mechanism in mid-thigh. J Orthop Sci 2017;22:99-104. [Google Scholar | PubMed]
- 10.Husebye ES, Anderson MS, Kämpe O. Autoimmune polyendocrine syndromes. N Engl J Med 2018;378:1132-41. [Google Scholar | PubMed]
- 11.Maheshwari AV, Yarmis SJ, Tsai J, Jauregui JJ. Progression of bisphosphonate-associated impending atypical femoral fracture despite prophylactic cephalomedullary nailing: A case report and review of literature. J Clin Orthop Trauma 2016;7:92-8. [Google Scholar | PubMed]
- 12.Anagnostis P, Paschou SA, Mintziori G, Ceausu I, Depypere H, Lambrinoudaki I, et al. Drug holidays from bisphosphonates and denosumab in postmenopausal osteoporosis: EMAS position statement. Maturitas 2017;101:23-30. [Google Scholar | PubMed]
- 13.Im GI, Lee SH. Effect of teriparatide on healing of atypical femoral fractures: A systemic review. J Bone Metab 2015;22:183-9. [Google Scholar | PubMed]
- 14.Lee SY, Niikura T, Iwakura T, Fukui T, Kuroda R. Clinical experience with the use of Low-Intensity Pulsed Ultrasound (LIPUS) in the treatment of atypical femoral fractures. J Orthop Trauma 2017;31:S2. [Google Scholar | PubMed]
- 15.Lovy AJ, Kim JS, Di Capua J, Somani S, Shim S, Keswani A, et al. Intramedullary nail fixation of atypical femur fractures with bone marrow aspirate concentrate leads to faster union: A case-control study. J Orthop Trauma 2017;31:358-62. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Minimally Invasive Prophylactic Plating for Bisphosphonate-induced Atypical Femoral Fracture Post Total Hip Replacement
March 1, 2026 Minimally Invasive Prophylactic Plating for Bisphosphonate-induced Atypical Femoral Fracture Post Total Hip Replacement September 10, 2023 Denosumab-associated Periprosthetic Atypical Femur Fracture: A Case Report
September 10, 2023 Denosumab-associated Periprosthetic Atypical Femur Fracture: A Case Report January 1, 2025 Fragment-specific Plate Fixation in a Case of Mayo Type IIB Olecranon Fracture: A Case Report
January 1, 2025 Fragment-specific Plate Fixation in a Case of Mayo Type IIB Olecranon Fracture: A Case Report April 10, 2024 Utility of Asymmetric Multilevel Pontes Osteotomy in Ankylosing Spondylitis with Scoliosis using Ultrasonic Bone Scalpel: Case Report
April 10, 2024 Utility of Asymmetric Multilevel Pontes Osteotomy in Ankylosing Spondylitis with Scoliosis using Ultrasonic Bone Scalpel: Case Report