
Cervical spondylolysis can be successfully treated conservatively in very young children with non-invasive approaches.
Dr. Claudio Silveri, Musculoskeletal Oncology Pathology Unit, Traumatology and Orthopedics Clinic of UdelaR at the National Institute of Orthopedics and Traumatology, Montevideo, Uruguay. E-mail: claudio.silveri@gmail.com
Abstract
Introduction: Cervical spondylosis is a rare condition in pediatric patients with currently scarce cases in the literature. The C2 location is particularly uncommon with only a small number of case reports describing this condition. Given its limited evidence in the literature, its etiology and standard of care treatment persist obscure.
Case Report: Here, we present the case of a 2-year-old with bilateral atraumatic C2 spondylolysis. The patient presented with initial negative radiographs and was later diagnosed with advanced imaging, emphasizing the importance of maintaining a high degree of suspicion in this setting. The patient underwent successful conservative treatment confirmed clinically and radiologically.
Conclusion: Cervical spondylolysis is uncommon in the pediatric population, the C2 location being particularly rare. Clinical presentation can be diverse ranging from asymptomatic to spine instability with associated neurological deficits. The diagnosis of this condition is challenging and there are no current strong recommendations regarding the treatment gold standard.
Keywords: Cervical spondylolysis, pediatric spondylolysis, C2 spondylolysis.
Cervical spondylosis is a rare condition in pediatric patients with currently scarce cases in the literature [1,2]. Spondylolysis refers to a structural defect, unilateral or bilateral, in the posterior arch of the vertebra, specifically in the pars articularis [3]. Most patients are adults and have an asymptomatic presentation. Those patients with symptoms often complain of pain, torticollis, or even neurological deficits arising from the associated spinal mechanical instability [4,5]. For the majority of cervical cases of spondylolysis, the defect is at the C6-C7 level and in decreasing frequency in C5 and C4 [6]. The C2 location is particularly uncommon with only a small number of case reports describing this condition [1,7-9]. Given its limited evidence in the literature, its etiology and standard of care treatment persist obscure. Furthermore, for many patients, the actual cause of the spondylolysis will remain unknown. Some authors suggest a congenital origin, with a defect in the ossification as the originating event [10]. This can be especially true when associated with other vertebral malformations. Traumatic etiology has been also described in adults as well as pediatric patients. Other hypotheses include repetitive microtrauma between two contiguous vertebras and non-union from a birth-related fracture [11]. Here, we describe the case of a 2-year-old male with a C2 spondylolysis of unknown origin with successful conservative treatment. This case portrays the difficulties associated with this challenging diagnosis from a clinical and radiologic standpoint.
A 2-year-old male, with no prior medical history, presented to the emergency department due to a complaint of 3 days of torticollis. Per the parents, no trauma had occurred previously nor the patient had any recent upper respiratory infections. Upon physical examination, the patient was noted to have painful torticollis with the neck rotated and flexed laterally in a fixed position. The rest of the physical examination was without abnormalities. A radiograph of the neck was then requested where no anomalies were found (Fig. 1). The patient was then discharged home with symptomatic treatment. The patient returned 3 days later due to the persistence of the same symptoms. A magnetic resonance imaging was then obtained, which demonstrated a subtle abnormality of the posterior arch of C2, with no signs of acute trauma (Fig. 2).
In addition, a computed tomography (CT) scan without contrast was also performed confirming bilateral spondylolysis of C2 (Fig. 3). Due to the uncertain etiology of the spondylolysis in this scenario and the absence of instability or neurological deficits, a decision was made to recommend conservative treatment with a cervical collar and serial radiographic controls.

A month after the initial symptoms, the patient was seen in the clinic presenting with a resolution of the torticollis and having only mild pain. A new radiograph was obtained which demonstrated now conspicuous bilateral spondylosis with a 3-mm gap noted in the pars articularis as well as a minimal C2 spondylolisthesis (Fig. 4). 
Radiographs and clinical controls continued until the lysis was confirmed to have resolved. Three months after the presentation, the patient had a complete resolution of his symptoms. A decision was made to remove the cervical collar and obtain a new CT scan, which showed notable callus peri-lysis (Fig. 5). During the 4-month follow-up, functional radiographs were performed, showing no cervical instability. At final control, 5 months from presentation, the patient had complete resolution of symptoms, had resumed all activities, and had a final radiograph and CT scan demonstrating full healing of the bilateral spondylolysis (Fig. 6).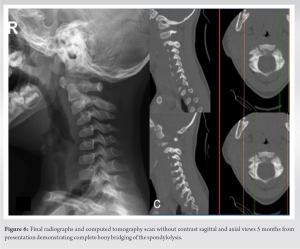
Spondylolysis at the C2 level is a rare condition with limited evidence regarding the pathology or its gold-standard treatment [1,12]. The etiology remains unknown; however, several hypotheses have been considered. A traumatic origin is usually contemplated in most cases, along with a congenital cause in the setting of very young patients [13-15]. Given obtaining an accurate history from young children can be challenging, the physician must assess the context to consider the possibility of non-accidental trauma [16]. Radiographic images, depending on the lysis edges features, can at times orient toward a congenital diagnosis; however, such findings are merely suggestive and not pathognomonic [1,17]. In the case of our patient, the findings are inconclusive. No conspicuous lysis edges are present to suggest a congenital etiology nor are present any additional signs to indicate an acute traumatic inciting event, such as hematoma or local edema surrounding the pars articularis. Moreover, the parents denied any history of trauma and the pediatrics team ruled out non-accidental trauma. There are no guidelines dictating the gold-standard treatment for pediatric cervical spondylolysis. In the literature, reports of individual asymptomatic cases have been treated conservatively with observation [17]. Additional symptomatic cases presenting symptoms or having a clear traumatic etiology are described as being treated with a cervical collar for a variable length of time [2,16]. Mechanical instability per se has not been considered an absolute indication for surgery, even though some recommend considering it [18,19]. Spinal instability has been described as presenting persistence of pain as well as neurological deficits and increasing displacement on dynamic radiographs [13,15,20]. Our patient did not present clinical instability nor did it demonstrate any propagation of the lysis during the observation period. Furthermore, on dynamic radiographs, no instability was present. In this setting of a stable lesion clinically and radiographically, a decision was made to proceed with conservative treatment with the aim of achieving bony consolidation of the lysis. A series of patients have shown that most patients are treated successfully with conservative treatment, with surgery being indicated in a small percentage of patients [16,18]. Our patient had a significant improvement with the use of a cervical collar for 12 weeks, even showing complete pain resolution at the 6-week follow-up. Similarly, imaging improvement was also noticed with the presence of a bony callus around the lysis. At the 20-week imaging control, complete bony healing was present.
Pediatric C2 spondylolysis is an extremely rare condition. Establishing a diagnosis as well as an etiology can oftentimes be challenging. Strict clinical and radiographic follow-ups are relevant for the appropriate treatment of these young patients. Here, we presented the case of a 2-year-old male with C2 spondylolysis of uncertain etiology. The patient was treated successfully with conservative treatment, achieving complete resolution of symptoms along with an ad integrum repair of the bony defect.
The key takeaway from the article on successful conservative treatment of cervical spondylolysis in a 2-year-old patient underscores the efficacy of non-invasive approaches in managing spinal conditions even in very young children. By employing methods such as bracing and careful monitoring, clinicians were able to achieve positive outcomes without resorting to surgical intervention. This case highlights the importance of early diagnosis, personalized care, and a multidisciplinary approach in addressing complex spinal issues in pediatric patients, showcasing the potential for conservative measures to yield favorable results in challenging cases.
References
- 1.Gressot LV, Vadivelu S, Hwang SW, Fulkerson DH, Luerssen TG, Jea A. Spondylolysis of C-2 in children 3 years of age or younger: Clinical presentation, radiographic findings, management, and outcomes with a minimum 12-month follow-up. J Neurosurg Pediatr 2014;13:196-203. [Google Scholar | PubMed]
- 2.Gottfried ON, Parker SL, Omeis I, Bydon A, Gokaslan ZL, Wolinsky JP. Spondylolysis of C-2 in 2 athletically active individuals. J Neurosurg Spine 2010;13:17-23. [Google Scholar | PubMed]
- 3.Berger RG, Doyle SM. Spondylolysis 2019 update. Curr Opin Pediatr 2019;31:61-8. [Google Scholar | PubMed]
- 4.Mohile NV, Kuczmarski AS, Lee D, Warburton C, Rakoczy K, Butler AJ. Spondylolysis and isthmic spondylolisthesis: A guide to diagnosis and management. J Am Board Fam Med 2022;35:1204-16. [Google Scholar | PubMed]
- 5.Kelly JC, Groarke PJ, Butler JS, Poynton AR, O’Byrne JM. The natural history and clinical syndromes of degenerative cervical spondylosis. Adv Orthop 2012;2012:393642. [Google Scholar | PubMed]
- 6.Kuo DT, Tadi P. Cervical spondylosis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/nbk551557 [Last accessed on 2023 May 01]. [Google Scholar | PubMed]
- 7.Currarino G. Primary spondylolysis of the axis vertebra (C2) in three children, including one with pyknodysostosis. Pediatr Radiol 1989;19:535-8. [Google Scholar | PubMed]
- 8.Fardon DF, Fielding JW. Defects of the pedicle and spondylolisthesis of the second cervical vertebra. J Bone Joint Surg Br 1981;63B:526-8. [Google Scholar | PubMed]
- 9.Hasue M, Kikuchi S, Matsui T, Machida H, Kurokawa T, Kataoka O. Spondylolysis of the axis. Report of four cases. Spine (Phila Pa 1976) 1983;8:901-6. [Google Scholar | PubMed]
- 10.Howard AW, Letts RM. Cervical spondylolysis in children: Is it posttraumatic? J Pediatr Orthop 2000;20:677-81. [Google Scholar | PubMed]
- 11.Hanakita J, Kondo A, Suzuki T. No Shinkei Geka. 1985;13(10):1097-1101. [Google Scholar | PubMed]
- 12.Ibebuike K, Roussot M, Watt J, Dunn R. Management challenges of traumatic spondylolisthesis of the Axis with an unusual C2-C3 posterior subluxation in a paediatric patient: Case report and literature review. Afr Health Sci 2018;18:458-67. [Google Scholar | PubMed]
- 13.Fedorchuk C, Comer RD, Stockwell TL, Stockwell J, Stockwell R, Lightstone DF. Prevalence of cervical spondylolisthesis in the sagittal plane using radiographic imaging in a pediatric population: A cross sectional analysis of vertebral subluxation. J Radiol Case Rep 2021;15:1-18. [Google Scholar | PubMed]
- 14.Kushare IV, Colo D, Kadhim M, Dormans JP. Bilateral C6 spondylolysis with spondylolisthesis in 3 adolescent siblings. J Pediatr Orthop 2014;34:e40-3. [Google Scholar | PubMed]
- 15.Legaye J, Horduna M. Cervical spondylolysis in a child: A case with hypermobility. Spine J 2009;9:e15-9. [Google Scholar | PubMed]
- 16.Samples DC, Staulcup S, Hovis G, Gustin P, Meier M, Mirsky D, et al. Refining the role of cervical spine immobilization and stabilization in pediatric non-accidental trauma, a retrospective series of 1008 patients. Childs Nerv Syst 2022;38:2357-64. [Google Scholar | PubMed]
- 17.Viana SL, Viana MA, de Alencar EL. Atypical, unusual, and misleading imaging presentations of spondylolysis. Skeletal Radiol 2015;44:1253-62. [Google Scholar | PubMed]
- 18.Goetzinger S, Courtney S, Yee K, Welz M, Kalani M, Neal M. Spondylolysis in young athletes: An overview emphasizing nonoperative management. J Sports Med (Hindawi Publ Corp) 2020;2020:9235958. [Google Scholar | PubMed]
- 19.Nishimura Y, Ellis MJ, Anderson J, Hara M, Natsume A, Ginsberg HJ. Progressively unstable C2 spondylolysis requiring spinal fusion: Case report. Neurol Med Chir (Tokyo) 2014;54:761-7. [Google Scholar | PubMed]
- 20.Farah K, Pech-Gourg G, Graillon T, Scavarda D, Fuentes S. A new minimally invasive technique for primary unstable C2 spondylolysis in an 8-year-old child: A case report and review of the literature. World Neurosurg 2018;115:79-84. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2018 The Challenges of the Femoral Bone Loss in the Management of the Floating Knee IIB According Fraser: A Case Report
January 10, 2018 The Challenges of the Femoral Bone Loss in the Management of the Floating Knee IIB According Fraser: A Case Report August 10, 2020 Gossypiboma: What Happens When a Mop is Left in a Thigh for ten Years
August 10, 2020 Gossypiboma: What Happens When a Mop is Left in a Thigh for ten Years May 23, 2018 Simultaneous Metacarpophalangeal Dislocation and Carpometacarpal Fracture-Dislocation of the Ring Finger: A Case Report
May 23, 2018 Simultaneous Metacarpophalangeal Dislocation and Carpometacarpal Fracture-Dislocation of the Ring Finger: A Case Report February 10, 2021 Bizarre Parosteal Osteochondromatous Proliferation (Nora Lesion) in Upper and Lower Limbs: A Report of Three Cases and Review of Literature
February 10, 2021 Bizarre Parosteal Osteochondromatous Proliferation (Nora Lesion) in Upper and Lower Limbs: A Report of Three Cases and Review of Literature