
• There is a variant of cervical spine predominant ankylosing spondylitis, where the disease activity commences and predominantly affects the cervical spine before involving the lumbar spine and sacroiliac joints which are commonly affected in a typical case of ankylosing spondylitis • The treatment and physiotherapy management for cervical spine predominant ankylosing spondylitis needs further refinement and research as the treatment for the traditional ankylosing spondylitis cannot be applied here.
Dr. S Venkatesh Kumar, MS DNB Orthopaedics MNAMS, Assistant Professor, Department of Orthopaedics, Dhanalakshmi Srinivasan Medical College and Hospital, Siruvachur, Perambalur - 621113, Tamil Nadu, India. E-mail: mailvenkatesh91@gmail.com
Introduction: Ankylosing spondylitis (AS) is a chronic, inflammatory disease of the axial spine characterized by the involvement of the spine and sacroiliac (SI) joints. Increasing spinal stiffness and persistent back pain are the most typical symptoms of this systemic illness. The most often affected areas in AS are the lumbosacral spine and the sacroiliac joints.
Case Report: We report this uncommon case of a 30-year-old male patient recently diagnosed with AS having an exclusive cervical spine involvement corroborated by X-rays and magnetic resonance imaging.
Conclusion: The results of the lumbosacral spine, fingers, chest, and sacroiliac joint examinations were normal. The examination of the sacroiliac joint, lumbosacral spine, chest, and digits was normal. The pain and neck stiffness were partially relieved by pharmacotherapy (NSAIDS) and physiotherapy. This is a rare presentation of AS, the reported literature on such case reports are very rare.
Keywords: Recently diagnosed ankylosing spondylitis, young male patient: exclusive cervical spine involvement.
Ankylosing spondylitis (AS) is a type of long-term inflammatory axial spondyloarthritis that is marked by inflammation of the sacroiliac and vertebral joints. It often starts with the pathology of the lumbar spine and the sacroiliac joint. The main clinical characteristic of AS is persistent back pain that affects the pelvis and the lower spine [1]. Classically, women and patients with long-term illnesses are more likely to have cervical spine involvement [2, 3]. Thus, we report this unique isolated cervical spine involvement in a 30-year-old male patient with early-onset AS.
A male patient in his 30s presented with the complaint of gradually progressive neck pain, which was associated with progressive stiffening with on-and-off mild-grade fever for 6 months. He had no prior history of diabetes, hypertension, or falls. He denied having myalgia, jaw claudication, blurred vision, diarrhea, or urethritis in the past. There is no such illness recorded in his family. Physical examination revealed normal body temperature and vitals on the day of the hospital visit. No skin rash was observed systemically. No tenderness was noted in the scalp and bony landmarks with tendon attachments in the body. A cervical spine examination revealed a stooping forward position of the neck and diffused mild tenderness. The cervical spine range of movements was 0–15° of flexion, 0–20° of lateral flexion, almost nil extension, and neck rotation possible (Fig. 1). However, the range of movements of the lumbar spine was normal with no complaints of stiffness. Moreover, there was no tenderness over the sacroiliac joints. His chest expansion was 5 cm and Schober’s test was negative.

Investigations
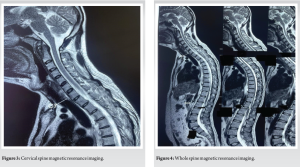
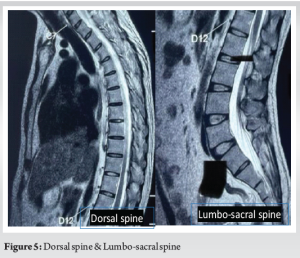
The laboratory values showed normal hemoglobin, leukocyte, and platelet counts along with normal liver and renal function tests. However, the CRP and ESR were above normal. Rheumatoid factor, anticyclic citrullinated peptide antibody, and antinuclear antibodies were negative. The human leukocyte antigens (HLA) B27 test was found to be positive. The cervical spine radiograph in lateral view demonstrated small erosions at the vertebral body corners and multiple syndesmophytes at C2 to C7 levels (Fig. 2). The magnetic resonance imaging (MRI) confirmed X-ray findings, and additionally, syndesmophyte at cervicothoracic junction C7/T1 was noted (Fig. 3). However, there were no signs of syndesmophytes in other levels of the thoracic/lumbar/lumbosacral region in the MRI (Fig. 4). On pelvic MRI, there was no sacroiliac joint inflammation noted or enthesitis noted.
Treatment
For the patient, we started non-steroidal anti-inflammatory (NSAID) medication. The patient received comprehensive home-based physiotherapy aimed at improving posture, enhancing mobility, and decreasing morning stiffness. To facilitate early diagnosis and treatment, the patient was also informed about the potential for future involvement of the rib cage, fingers, lumbosacral joint, and sacroiliac joint. The patient was routinely checked on and his adherence to physiotherapy and medication was monitored. (Fig. 5)
Outcome and follow-up
The Bath Ankylosing Spondylitis Disease Activity Index was 3. The Bath Ankylosing Spondylitis Metrology Index and Bath Ankylosing Spondylitis Functional Index scores were 5. After receiving regular medication and physical therapy, the patient’s cervical pain was better on and off. The cervical spine’s stiffness partially improved. For personal reasons, the patient did not receive therapy for 2 weeks, during which time he noticed a return of the pain and stiffness.
The sacroiliac joint is typically where the inflammatory disease process in AS begins [4]. At every stage of the disease’s progression, a greater number of patients had lumbar involvement than cervical disease, according to Brophy et al. [5] who also proposed that lumbar spine involvement comes before cervical disease. Cervical spine involvement is common among women and in patients with a long-duration AS [2, 3]. Similarly, El Maghraoui et al. [6] report that cervical spine involvement in AS is more common in symptomatic and structurally severe forms of the disease and increases with age and duration of the condition. Clinical and radiological involvement were statistically significantly consistent with each other in AS. According to Jang et al. [7] in cases of isolated cervical involvement, men and women were equally likely to experience cervical-predominant involvement at a similar frequency. Nonetheless, Resnick et al. [3] and Meijers et al. [2] discovered that radiological alterations in the cervical spine were more prevalent in women with AS. AS exhibits a hereditary component and has been linked to ulcerative colitis, Reiter’s syndrome, and other gastrointestinal disorders. Low back discomfort is the most typical presenting symptom [8]. However, in our situation, neck pain and stiffness were the main complaints. In addition, we discovered radiographic alterations that matched those seen in earlier research and suggest that lumbar radiographic results usually come before cervical findings [9]. Jang et al. [7] indicate that the involvement of the cervical spine was not as noticeable until 20 years or more into the disease, with a predominance of the lumbar over the cervical spine. Research has indicated that while 1%–2% of HLA-B27-positive people go on to develop AS, 90%–95% of AS patients are HLA-B27 positive. This percentage rose to 15%–20% for people who had a first-degree relative who was impacted [10]. HLA-B27-positive individuals had a much lower age of disease onset than HLA-B27-negative patients. The first-line medications are non-steroidal anti-inflammatory medicines (NSAIDs), which successfully reduce symptoms. At present, biological medicines such as infliximab have been employed in hopes of addressing the underlying inflammatory process. Our patient had mild-to-moderate pain relief from NSAIDS along with a patient-specific physiotherapy regimen. The patient was routinely checked and found that the pain and stiffness were better as long as the patient was adherent to the treatment plan.
A predominant cervical spine involvement is a rare entity in AS. The literature research on which seems to be rare and this area is underexplored. This case report indicates that there are other clinical variants of AS and indicates the need for further research on AS-predominant cervical spine variants where the current treatment regime, physiotherapy, and rehabilitation give moderate if not unsatisfactory results to the current treatment and rehabilitation regime. The treatment regime in such clinical variants of AS needs further improvement/modification to improve disease outcome, functional recovery, and pain relief which should be planned according to the patient’s specific needs.
The literature research on early cervical spine involvement in AS that too in a young male patient who was recently diagnosed with AS where there is no clinical or radiological involvement of other typically affected areas of the spine is rare and not reported.
References
- 1.Sampaio-Barros PD, Bertolo MB, Kraemer MH, Neto JF, Samara AM. Primary ankylosing spondylitis: Patterns of disease in a Brazilian population of 147 patients. J Rheumatol 2001;28:560-5. [Google Scholar]
- 2.Meijers KA, Van Voss SF, François RJ. Radiological changes in the cervical spine in ankylosing spondylitis. Ann Rheum Dis 1968;27:333-8. [Google Scholar]
- 3.Resnick D, Dwosh IL, Goergen TG, Shapiro RF, Utsinger PD, Wiesner KB, et al. Clinical and radiographic abnormalities in ankylosing spondylitis: A comparison of men and women. Radiology 1976;119:293-7. [Google Scholar]
- 4.Peh Wilfred CG. Ankylosing Spondylitis. Emedicine; 2009. Available from: https://emedicine.medscape.com/article/386639 [Last accessed on 2010 Apr 18]. [Google Scholar]
- 5.Brophy S, Mackay K, Al-Saidi A, Taylor G, Calin A. The natural history of ankylosing spondylitis as defined by radiological progression. J Rheumatol 2002;29:1236-43. [Google Scholar]
- 6.El Maghraoui A, Bensabbah R, Bahiri R, Bezza A, Guedira N, Hajjaj-Hassouni N. Cervical spine involvement in ankylosing spondylitis. Clin Rheumatol 2003;22:94-8. [Google Scholar]
- 7.Jang JH, Ward MM, Rucker AN, Reveille JD, Davis JC Jr., Weisman MH, et al. Ankylosing spondylitis: Patterns of radiographic involvement--a re-examination of accepted principles in a cohort of 769 patients. Radiology 2011;258:192-8. [Google Scholar]
- 8.Sieper J, Braun J, Rudwaleit M, Boonen A, Zink A. Ankylosing spondylitis: An overview. Ann Rheum Dis 2002;61 Suppl 3:iii8-18. [Google Scholar]
- 9.Gran JT, Skomsvoll JF. The outcome of ankylosing spondylitis: A study of 100 patients. Br J Rheumatol 1997;36:766-71. [Google Scholar]
- 10.Brown MA. Genetics of ankylosing spondylitis. Curr Opin Rheumatol 2010;22:126-32. [Google Scholar]








