The aim of this case presentation is to bring awareness to atypical locations of these ACJ cysts that can be easily interpreted as a tumoral process in the neck due to the location of the mass.
Dr. Gregory Cunningham, Department of Orthopaedic Surgery and Traumatology, Centre Epaule Coude La Colline: Chem. Thury 7b, 1206 Geneva, Switzerland. E-mail: gregory.cunningham@cepco.ch
Introduction: Acromioclavicular joint cysts represent a relatively rare clinical entity, often manifested as an enlarging mass adjacent to the acromioclavicular joint, which can raise concerns for a potential tumor. These cysts are identified for their association with shoulder pathology, particularly extensive rotator cuff tears, and present a diagnostic and therapeutic challenge for misdiagnosis as neoplastic masses. In this case, we are reporting on an unusual presentation of a patient presenting with a swollen mass in the left trapezius causing neck pain. The aim of this case presentation is to bring awareness to atypical locations of these acromioclavicular joint cysts that can be easily interpreted as a tumoral process in the neck due to the location of the mass. Acromioclavicular cysts remain infrequently reported in the literature.
Case Report: We present the case of an 80-year-old male patient. On clinical examination, a soft and palpable mass over the trapezius was noted, with no signs of infection or inflammation. Plain radiographs showed advanced primary osteoarthritis of the glenohumeral joint with a preserved subacromial space. Magnetic resonance imaging of both shoulders showed that cystic masses were developed on both sides from the acromioclavicular joint and extended medially to the trapezius muscles. It was particularly large on the left side, with a diameter reaching up to 12 cm. The surgical intervention was carried out involving resection of the distal end of the clavicle through an open approach and resection of the neck of the cyst. Through a second incision at the dorsal level on the medial aspect of the trapezius, the cyst sac was identified and its subsequent resection was performed.
Conclusion: The presented case of a rare location of bilateral ACJ cysts, treated successfully with cyst resection and ACJ decompression, illustrates a diagnostic and therapeutic challenge due to the atypical nature of the cysts’ presentation. This case aims to bring awareness about this pathology when confronted with a painless lump in the upper shoulder region, although far away from the joint in patients with complex shoulder or neck symptomatology.
Keywords: Acromioclavicular cyst, neck mass, shoulder pain, acromioclavicular joint, rotator cuff tear, shoulder tumor.
Acromioclavicular joint (ACJ) cysts represent a relatively rare clinical entity, often manifested as an enlarging mass adjacent to the AC joint, which can raise concerns for a potential tumor [1, 2]. These cysts are identified for their association with shoulder pathology, particularly extensive rotator cuff tears, and present a diagnostic and therapeutic challenge for misdiagnosis as neoplastic masses [3, 4]. The management of ACJ cysts ranges from conservative observation to surgical intervention, including aspiration with a high risk of recurrence, cyst excision, and in some cases, excision of the AC joint itself coupled with repair of any underlying rotator cuff abnormalities if possible. In this case, we are reporting on an unusual presentation of a patient presenting with a swollen mass in the left trapezius causing neck pain. The aim of this case presentation is to bring awareness to the atypical locations of these ACJ cysts that can be easily interpreted as a tumoral process in the neck due to the location of the mass. ACJ cysts remain infrequently reported in the literature, with 77 cases documented in the literature and only three cases have been reported with this atypical location in the trapezius muscle.
We present the case of an 80-year-old male patient who is a healthy active regular swimmer. He had no significant past medical history, apart from bilateral rotator cuff repair over 15 years ago, with mild pain on the left side successfully treated with a glenohumeral injection. He was concerned about a growing lump in the left trapezius muscle over the last 6 months with mild pain in the neck. There were no chills, fever, loss of appetite, or weight associated with it, and no history of trauma or wounds in this location. On clinical examination, a soft and palpable mass over the trapezius was noted, with no signs of infection or inflammation. Shoulder range of motion and strength were preserved with some crepitus, except for internal rotation which came to L5 against Th8 with a weak Lift-Off test (Fig. 1 and 2).

Clinically, a mass is observed on his left trapezius with no clear signs of tracking from the ACJ. Plain radiographs showed advanced primary osteoarthritis of the glenohumeral joint with a preserved subacromial space (Fig. 3 and 4), as well as severe ACJ arthropathy. Magnetic resonance imaging (MRI) of both shoulders showed severe synovitis and effusion in the glenohumeral joint extending to the bursa through bilateral massive rotator cuff tears. Cystic masses were developed on both sides from the ACJ and extended medially to the trapezius muscles. It was particularly large on the left side, with a diameter reaching up to 12 cm (Fig. 5 and 6).
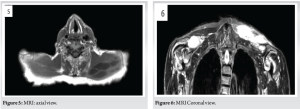
Progression of signs of osteoarthritis with narrowing of the joint space and osteophytic changes. Fine diffuse calcifications within the rotator cuff. Axial view of the left cyst which is clearly going through between the muscle fibers of the trapezius colonized by the synovitis. Confirmation of a cystic formation with an arthrosynovial appearance, measuring 12 cm in its largest diameter within the left trapezius, appearing to connect to the left acromioclavicular joint itself, in communication with the subacromial bursa and the underlying glenohumeral joint. Given the size of the cyst and the patient’s concerns about persistent symptoms, a surgical approach was considered. Treatment options were discussed, including a reverse shoulder prosthesis, cyst resection, and acromioclavicular decompression with resection of the distal end of the clavicle. Given the mild symptoms and functional restrictions in the left shoulder, the decision was made to proceed with cyst resection and acromioclavicular decompression. The surgical intervention was carried out without complications, involving resection of the distal end of the clavicle through an open approach and resection of the neck of the cyst that was identified as arising from the joint (Fig. 7). Through a second incision at the dorsal level on the medial aspect of the trapezius, the cyst sac was identified and its subsequent resection was performed (Fig. 8). The content was mucoid clear liquid and was sent for bacteriologic analyses that came back negative.
Resection of the superior capsule and neck of the cyst.
ACJ was exposed (Arrow), and a second incision was made over the axis of the sac of the cyst (*).
As per the final follow-up at 3 months, the patient has no experienced shoulder or neck symptoms and there are no signs of recurrence (Fig. 9 and 10). No recurrence, absence of mass, and good healing of the incisions.

ACJ cysts most often present as enlarging masses adjacent to the AC joint (Geyser sign) and can be pauci- or asymptomatic. This is what has been published in the literature. However, our case is the fourth case published up-to-date (4 out of 77), where the cyst is not located over the ACJ and this atypical location in the trapezius can be easily interpreted as a tumoral process in the neck not related to the shoulder.
Classification and pathogenesis
AC joint cysts are categorized into two main types, reflecting their underlying pathophysiology. Type 1 cysts emerge primarily from degenerative changes within the AC joint, attributable to factors such as trauma, infection, metabolic disease, or repetitive use. These cysts remain confined to the joint area without involvement of the rotator cuff. The pathogenesis involves long-term degeneration leading to synovial inflammation and subsequent cyst formation [3]. Conversely, Type 2 cysts are a consequence of chronic rotator cuff tears, where the superior migration of the humeral head impinges on the AC joint. This results in degeneration and the formation of a cyst, the degenerate ACJ essentially acts like a one-way valve, allowing synovial fluid to escape from the GHJ into the cyst but otherwise prevents back-flow [3]. After a meticulous review of the literature, 69 cases of Type 2 cysts have been published (89.6%) and there are only eight cases of Type 1 cysts (10.4%). The case under consideration illustrates a scenario where a rotator cuff tear coexists, aligning it with Type 2 cysts. Montet et al. also proposed a theory suggesting that AC joint cysts could result from chronic instability of the joint due to massive rotator cuff tears. Their observation that ganglia can dissect inside muscles challenges traditional theories and underscores the need for a nuanced understanding of AC joint cyst pathogenesis. However, the theory proposed by Craig is widely accepted, Montet et al. suggest that it cannot explain the cyst mucoid content and fibrous wall [5].
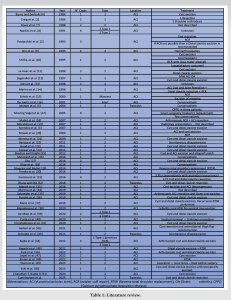
A literature review based on a PubMed database search conducted in March 2024 with the title “Acromioclavicular joint cyst” “ACJ cyst” and “Acromioclavicular joint ganglion”. The literature surrounding acromioclavicular (AC) joint cysts has been published since 1984, contributing to our understanding of the complexity and varied presentations of this pathology. ACJ cysts remain infrequently reported in the literature, with only 77 documented cases, and of those 77, only 3 cases (3.8%) were located in the trapezius muscle. Another two cases were reported as a mass at the ACJ, where the mass was identified as a myxoma in one case, and as gout deposits in a second case (Table 1).
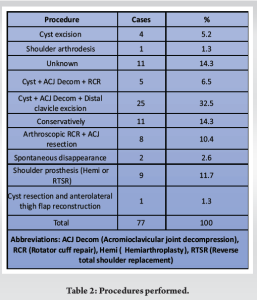
Successful treatment involved excision of the cyst, resection of the distal clavicle, and repair of the torn cuff. The importance of addressing both the cyst and the underlying pathology, when possible, for favorable outcomes is well known [1, 2]. In recent years, arthroscopic excision of the cyst and distal clavicle has been reported with satisfactory results [18, 35, 44, 46, 50]. Excision of the cyst and resection of the distal clavicle was the most common procedure with 25 cases of a total of 78 cases (32.5%), eight cases were treated arthroscopically (10.4%), 11 cases were treated conservatively (14.3%), and nine cases were treated with shoulder replacement, hemiarthroplasties or reverse total shoulder replacement (RTSR) (11.7%) (Table 2).
Groh et al. treated four patients with chronic irreparable rotator cuff tears, degenerative arthritis of the glenohumeral joint, and associated cysts over the AC joint with shoulder hemiarthroplasties. This approach suggests that in certain cases, joint replacement may be a viable option for managing extensive AC joint pathology due to the increasing indication of reverse shoulder replacement in recent years [9, 29, 37, 45, 48]. Murena et al. reported the first case of a patient with an ACJ Type 2 cyst, who underwent four ultrasound-guided aspirations, and following the last aspiration the patient developed a fistula draining serous fluid from the puncture site. Therefore, Murena et al. given the high recurrence rate associated with this procedure and the increased risk of determining the formation of a fistula discourage multiple ACJ cyst aspirations [21]. A second case was reported by Emam et al. where the patient due to the fistula underwent a staged reverse total shoulder replacement [48]. Tham et al. described a case where after multiple aspirations the cyst increased in size [49]. Hartog et al. reported a case with spontaneous disappearance of an acromioclavicular joint cyst. Superior migration of the humeral head was a sign of rotator cuff tear. Two months after the first presentation, the symptoms were still minor, and the swelling had completely disappeared [22]. Montet et al. reported the first case of an intramuscular ganglion cyst located in the trapezius muscle arising from the AC joint and associated with a massive tear of the rotator cuff. This represents the first case reported in the literature describing an ACJ cyst, associated with cuff pathology that infiltrated the muscle belly of the trapezius rather than the subcutaneous tissue. Montet et al. treated conservatively the patient due to mild symptoms and minor limitations in the activities of daily life [5]. Zhang and Old was the second case reported of a cyst tracking to the trapezius muscle, which was resected, and a distal clavicle excision was performed with no recurrence after 3 months of follow-up [32], Spinnato et al. reported the third case to date with the atypical location into the trapezius muscle. The patient was treated with a corticoid injection due to comorbidities and after 8 months, a complete spontaneous remission was observed [43]. In our case, the patient presented with an atypical bilateral mass over the trapezius, with symptomatology on the left side. After confirming with MRI the atypical location of the cyst, a surgical resection of the cyst and the distal clavicle was performed with a double incision. As per the final follow-up at 3 months, the patient has no experienced shoulder or neck symptoms and there are no signs of recurrence.
The presented case of a rare location of bilateral ACJ cysts, treated successfully with cyst resection and ACJ decompression, illustrates a diagnostic and therapeutic challenge due to the atypical nature of the cysts’ presentation. This highlights the importance of comprehensive clinical and imaging evaluation in patients with complex shoulder or neck symptomatology. The aim of this case is to bring awareness about this pathology when confronted with a painless lump in the upper shoulder region, although far away from the joint. Moreover, this case contributes additional evidence to the medical literature on the manifestations and management options of acromioclavicular cysts and puts more emphasis on this atypical location as this case is the fourth case described in the literature.
This case report highlights the importance of considering acromioclavicular joint cysts in the differential diagnosis of neck masses, particularly those presenting as painless lumps in atypical locations such as the trapezius muscle. The case of an 80-year-old male with bilateral ACJ cysts extending into the trapezius, initially mimicking a tumoral process, illustrates the diagnostic challenges and potential for misdiagnosis associated with this rare pathology. Successful management through cyst resection and ACJ decompression highlights the necessity for awareness among orthopedic surgeons. Recognizing such atypical presentations can facilitate accurate diagnosis and appropriate treatment, ultimately improving patient outcomes. This report provides valuable insights that can aid orthopedic and general practitioners in effectively identifying and managing similar cases.
References
- 1.Craig EV. The acromioclavicular joint cyst: An unusual presentation of a rotator cuff tear. Clin Orthop Relat Res 1986;202:189-92. [Google Scholar]
- 2.Postacchini F, Perugia D, Gumina S. Acromioclavicular joint cyst associated with rotator cuff tear: A report of three cases. Clin Orthop Relat Res 1993;294:111-3. [Google Scholar]
- 3.Hiller AD, Miller JD, Zeller JL. Acromioclavicular joint cyst formation. Clin Anat 2010;23:145-52. [Google Scholar]
- 4.Kontakis GM, Tosounidis TH, Karantanas A. Isolated synovial cyst of the acromio-clavicular joint associated with joint degeneration and an intact rotator cuff. Acta Orthop Belg 2007;73:515-20. [Google Scholar]
- 5.Montet X, Zamorani-Bianchi MP, Mehdizade A, Martinoli C, Bianchi S. Intramuscular ganglion arising from the acromioclavicular joint. Clin Imaging 2004;28:109-12. [Google Scholar]
- 6.Burns SJ, Zvirbulis RA. A ganglion arising over the acromioclavicular joint: A case report. Orthopedics 1984;7:1002-4. [Google Scholar]
- 7.Rowe C. Symptomatic Cysts of the Acromioclavicular Joint. The Shoulder. New York: Churchill Livingstone; 1988. p. 644-5. [Google Scholar]
- 8.Nardini C. Sul significato delle cisti acromioclavicolari: Loso assocazone con la rottura della cuffia dei rotatori. Minerva Orthop 1991;7:211-6. [Google Scholar]
- 9.Groh GI, Badwey TM, Rockwood CA Jr. Treatment of cysts of the acromioclavicular joint with shoulder hemiarthroplasty. J Bone Joint Surg Am 1993;75:1790-4. [Google Scholar]
- 10.Utrilla AL, Gomez LM, Aznar AP, Gomez RC. Rotator cuff tear and acromioclavicular joint cyst. Acta Orthop Belg 1995;61:144-6. [Google Scholar]
- 11.Le Huec J, Zipoli B, Schaeverbeke T, Moinard M, Chauveaux D, Le Rebeller A. Acromio-clavicular joint cyst. Surgical treatment. Acta Orthop Belg 1996;62:107-12. [Google Scholar]
- 12.Segmüller HE, Saies AD, Hayes MG. Ganglion of the acromioclavicular joint. J Shoulder Elbow Surg 1997;6:410-2. [Google Scholar]
- 13.Selvi E, De Stefano R, Frati E, Manganelli S, Manca S, Marcolongo R. Rotator cuff tear associated with an acromioclavicular cyst in rheumatoid arthritis. Clin Rheumatol. 1998;17:170-1. [Google Scholar]
- 14.Marino AJ, Tyrrell PN, El-Houdiri YA, Kelly CP. Acromioclavicular joint cyst and rotator cuff tear. J Shoulder Elbow Surg 1998;7:435-7. [Google Scholar]
- 15.Echols PG, Omer GE Jr., Crawford MK. Juxta-articular myxoma of the shoulder presenting as a cyst of the acromioclavicular joint: A case report. J Shoulder Elbow Sur 2000;9:157-9. [Google Scholar]
- 16.De Santis D, Palazzi C, D’Amico E, Di Mascio DE, Pace‐Palitti V, Petricca A. Acromioclavicular cyst and “porcupine shoulder” in gout. Rheumatology 2001;40:1320-1. [Google Scholar]
- 17.Tshering Vogel DW, Steinbach LS, Hertel R, Bernhard J, Stauffer E, Anderson SE. Acromioclavicular joint cyst: Nine cases of a pseudotumor of the shoulder. Skeletal Radiol 2005;34:260-5. [Google Scholar]
- 18.Mullett H, Benson R, Levy O. Arthroscopic treatment of a massive acromioclavicular joint cyst. Arthroscopy 2007;23:446.e1-4. [Google Scholar]
- 19.Moratalla MB, Gabarda RF. Acromioclavicular joint ganglion. Eur J Radiol Extra 2007;63:21-3. [Google Scholar]
- 20.Nowak DD, Covey AS, Grant RT, Bigliani LU. Massive acromioclavicular joint cyst. J Shoulder Elbow Surg 2009;18:e12-4. [Google Scholar]
- 21.Murena L, D’Angelo F, Falvo DA, Vulcano E. Surgical treatment of an aseptic fistulized acromioclavicular joint cyst: A case report and review of the literature. Cases J 2009;2:8388. [Google Scholar]
- 22.Bas de Hartog M, Schimmel JW, Rijk PC. Spontaneous disappearance of an acromioclavicular joint cyst: A case report. Am J Orthop (Belle Mead NJ) 2011;40:367-8. [Google Scholar]
- 23.Good LM, DiCarlo JB, High WA. An unusual cutaneous manifestation of a ganglion cyst. J Am Acad Dermatol 2011;64:1206-8. [Google Scholar]
- 24.Cooper HJ, Milillo R, Klein DA, DiFelice GS. The MRI geyser sign: Acromioclavicular joint cysts in the setting of a chronic rotator cuff tear. Am J Orthop (Belle Mead NJ) 2011;40:E118-21. [Google Scholar]
- 25.Skedros JG, Knight AN. Massive acromioclavicular ganglionic cyst treated with excision and allograft patch of acromioclavicular region. J Shoulder Elbow Surg 2012;21:e1-5. [Google Scholar]
- 26.McCreesh KM, Riley SJ, Crotty JM. Acromio-clavicular joint cyst associated with a complete rotator cuff tear-A case report. Man Ther 2014;19:490-3. [Google Scholar]
- 27.Cho CH. Complicated acromioclavicular joint cyst with massive rotator cuff tear. Am J Orthop 2014;43:70-3. [Google Scholar]
- 28.Khor AY, Wong SB. Clinics in diagnostic imaging (151). Acromioclavicular joint geyser sign with chronic full-thickness supraspinatus tendon (SST) tear. Singapore Med J 2014;55:53-6. [Google Scholar]
- 29.Shaarani SR, Mullett H. Reverse total shoulder replacement with minimal ACJ excision arthroplasty for management of massive ACJ cyst-a case report. Open Orthop J 2014;8:298-301. [Google Scholar]
- 30.Tanaka S, Gotoh M, Mitsui Y, Shirachi I, Okawa T, Higuchi F, et al. A case report of an acromioclavicular joint ganglion associated with a rotator cuff tear. Kurume Med J 2016;63:29-32. [Google Scholar]
- 31.Gumina S, Candela V, Passaretti D. Acromioclavicular joint cyst in ASA 3-4 patients. Whether and how quickly it recurs after aspiration and steroid injection. Acta Orthop Belg 2016;82:161-5. [Google Scholar]
- 32.Zhang Y, Old J. Massive acromioclavicular joint cyst with intramuscular extension: Case report and review. Case Rep Orthop 2018;2018:7602549. [Google Scholar]
- 33.Maziak N, Plachel F, Scheibel M, Moroder P. Acromioclavicular joint cyst formation in a patient with rotator cuff-tear arthropathy: A rare cause of shoulder discomfort. BMJ Case Rep 2018;2018:bcr2018226188. [Google Scholar]
- 34.Martins P, Teixeira V, Saraiva F, Ponte C. The geyser sign: An unusual presentation of a rotator cuff tear. Acta Reumatol Port 2019;44:155-7. [Google Scholar]
- 35.Schneider KN, Gosheger G, Liem D. Progressive prominent swelling over the acromioclavicular joint. Dtsch Arztebl Int 2019;116:38. [Google Scholar]
- 36.Purohit S, Keny S, Raja B, Marathe N. Massive acromio-clavicular joint ganglion cyst associated with cuff tear arthropathy and acromioclavicular joint arthritis with normal functional shoulder-A case report. J Clin Orthop Trauma 2019;10:522-5. [Google Scholar]
- 37.Maris SJ, Tsiotsias A, Balfousias T, Angelis S, Kosmas L, Papatheodorou A, et al. An unusual presentation of a massive acromioclavicular joint ganglion cyst geyser sign secondary to massive rotator cuff tear and cuff arthropathy. J Long Term Eff Med Implants 2019;29:187-90. [Google Scholar]
- 38.Seet D, Manohara R, Hallinan JT, Tay SH. Geyser sign: Biomechanics and clinical implications. Ann Acad Med Singapore 2020;49:621-5. [Google Scholar]
- 39.Maio FD, Marcantonio AD, Luna VD, Caterini A, Tresoldi I, Farsetti P. Synovial cyst of the acromioclavicular joint with and without rotator cuff tear: A case series of two patients. Int J Surg Case Rep 2020;75:390-3 [Google Scholar]
- 40.Costa RP, Ramos J, Barroso J. Acromioclavicular cyst with geyser sign-An uncommon presentation of massive rotator cuff tear. Rehabilitación (Madr) 2021;55:238-40. [Google Scholar]
- 41.Christodoulou KC, Kakagia DD, Galanis VG, Tsoucalas GI, Fiska AT. Gigantic acromioclavicular joint cyst: Presentation and mini review. J Shoulder Elbow Surg 2021;30:e18-24. [Google Scholar]
- 42.Hattori Y, Imai S, Nakamura Hara R, Niu A. Acromioclavicular joint cyst treated with excision and anterolateral thigh flap reconstruction. Plast Reconstr Surg Glob Open 2021;9:e3412. [Google Scholar]
- 43.Spinnato P, Facchini G, Bazzocchi A, Errani C, Marinelli A. Acromioclavicular joint cyst with intramuscular extension presenting as a mass at the base of the neck. J Clin Rheumatol 2021;27:S457-9. [Google Scholar]
- 44.Kajita Y, Iwahori Y, Harada Y, Takahashi R, Deie M. Arthroscopic treatment of massive acromioclavicular joint ganglion cysts with color-aided visualization: A case series of 4 patients. JSES Rev Rep Techn 2022;2:526-34. [Google Scholar]
- 45.Higashi T, Mifune Y, Nishimoto H, Inui A, Hoshino Y, Matsushita T, et al. Kuroda, co-occurring acromioclavicular joint cyst and Hemarthrosis of the shoulder associated with rotator cuff tear arthropathy. Cureus 2022;14:e23353. [Google Scholar]
- 46.Fujii Y, Matsumura N, Furuhata R, Kimura H, Suzuki T, Iwamoto T, et al. Arthroscopic distal clavicle resection for an acromioclavicular ganglion cyst with cuff tear arthropathy: A case report. JBJS Case Connect 2022;12:e21. [Google Scholar]
- 47.Sayed AA, Alariefy M, Aldawsari M, Aljedani AN, Alharbi HH, Sayed A, et al. A case report of geyser sign on magnetic resonance imaging (MRI) in a 65-year-old female patient. Cureus 2022;14 :e23751. doi: 10.7759/cureus.23751. [Google Scholar]
- 48.Emam M, Singhani N, Persaud C, Aibinder W. Fistula of acromioclavicular cyst treated with a staged reverse total shoulder arthroplasty: A case report. BMC Musculoskeletal Disord 2022;23:1005. [Google Scholar]
- 49.Tham SY, Ng PH, Phua SK, Ho SW, Tham S. Aspiration of a large acromioclavicular joint cyst complicated by recurrence and enlargement: A case report. Cureus 2023;15:e34754. [Google Scholar]
- 50.Eckl L, Freislederer F, Toft F. Arthroscopic-assisted, joint preserving surgical treatment of a cuff tear arthropathy-related acromioclavicular joint cyst with associated geyser sign: A case report. JSES Rev Rep Tech 2023;3:230-5. [Google Scholar]
- 51.Chaudhari T, Gupta A. Acromioclavicular ganglion cyst: A rare case report. Cureus 2024;16:e54089. [Google Scholar]