
To understand the challenges in positioning and reducing intertrochanteric fracture in ipsilateral above-knee amputee and method to reduce and fix the fracture using a traction table.
Dr. Shaunak Sandeep Patwardhan, International Training Fellow (T&O), Department of Trauma and Orthopaedics, Salford Royal Hospital, Salford, Greater Manchester M6 8HD. E-mail: patwardhanshaunak@gmail.com
Introduction: Although commonly encountered in clinical practice and considered among the “bread and butter” cases in trauma and orthopedics, intertrochanteric fractures of the femur in certain scenarios pose a challenge to the orthopedic surgeon. Good reduction and stable fixation are a key for good outcome, and certain anatomical limitations such as amputations make that difficult to achieve. Ipsilateral above-knee amputation is a scenario where positioning of the patient on an orthopedic fracture table and reduction of the fracture becomes challenging.
Case Report: An active 59-year-old female with good functional baseline and ipsilateral above-knee amputation presented with an intertrochanteric fracture of the right proximal femur. The fracture was treated operatively and fixed with a dynamic hip screw (DHS). This case report highlights the technique of positioning of the patient and reduction of the fracture on a traction table using skeletal traction though the amputation stump with a Denham pin connected to the traction device.
Conclusion: This technique provides a reliable and stable means of reducing the fracture using skeletal traction through the bone itself and will be helpful to any orthopedic surgeon faced with a similar situation. This report also sheds light on current literature regarding different ways of overcoming the challenge of positioning and reducing intertrochanteric/intracapsular neck femur fractures using the orthopedic traction table in patients with ipsilateral limb amputations.
Keywords: Intertrochanteric fracture, above-knee amputation, reduction techniques, traction table
Intertrochanteric femur fractures are among the most common fractures encountered in orthopedic practice with a majority being seen in elderly patients [1]. The management of these fractures is invariably operative owing to the need for early mobilization of the patients and prevention of immobility-related complications. The common technique of surgical fixation is with the use of an orthopedic traction table and implants –either intramedullary nailing or dynamic hip screw (DHS) [2]. The orthopedic traction table is a device/attachment to operation tables which enables the injured limb to be placed and securely held in desired amounts of traction, rotation, elevation, abduction/adduction to achieve and maintain fracture reduction without the need for additional effort. The foot of the injured limb is placed in the traction boot attachment of the device and manipulated mechanically to achieve and maintain fracture reduction. However, in cases of amputation in the ipsilateral limb, positioning of the patient and reduction using the traction table becomes a challenge [3]. This case report highlights the reduction and surgical technique for fixation of an intertrochanteric femur fracture using a traction table in a 59-year-old lady with ipsilateral above-knee amputation.
A 59-year-old female patient presented to the Emergency Department having sustained a fall while chair skiing. The patient presented with pain in the right hip with restricted and painful movements. On examination, the right lower limb [stump] was externally rotated and active straight leg raise was not possible. Passive range of motion was painful and restricted. The patient had undergone a right above-knee amputation previously due to a complication of previous trauma resulting in malunion of the tibia and fibula along with severe CRPS. The amputation stump was healthy and well healed. There was no neurovascular deficit distal to the injury and no wound on the skin around the injury. The patient was non-compliant with the use of a prosthesis due to hypersensitivity at the stump and was using a wheelchair to mobilize before the fall. She was reasonably active and would occasionally use crutches to walk. She lived alone and was self-reliant and also engaged in activities such as gardening and swimming. Considering this background, the patient wanted to get back to her pre-injury functional level at the earliest possible.
Investigations
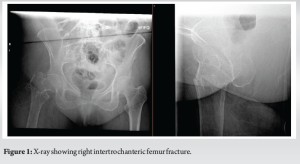
The patient was investigated as per the trauma protocol. X-rays of the lumbar spine, pelvis and right and the entire length of the amputation stump were performed along with a chest X-ray to check for rib injuries. Routine pre-operative blood investigations were done. The X-rays showed a comminuted extracapsular intertrochanteric femur fracture on the right side with impaction and varus angulation (Fig. 1). The hip joints on both sides showed mild degenerative changes.
Based on the history of acute trauma (fall) coupled with the clinical examination findings and evidence of fracture as seen on the X-ray, the diagnosis of intertrochanteric fracture was confirmed. The fact that there was an ipsilateral above-knee amputation with limited weight bearing on that limb gives more reason for the patient to sustain a fracture in that limb due to weakening of bone caused by chronic disuse. Other factors to consider in such cases would be pathological fractures due to either infection or malignancy. However, there were no factors suggestive of either infection or malignancy leading to a pathological fracture.
Treatment
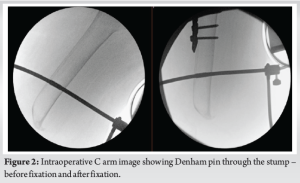
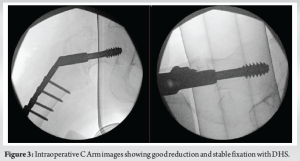
Considering poor quality of bone in this case due to disuse osteoporosis, previous history of CRPS leading to above-knee amputation, and surgical difficulty in positioning, reduction, and fixation due to the amputation, the option of conservative management was also discussed with patient. However, considering patients functional baseline, wish for early return to function and for relief of pain in the short-term decision for surgical fixation was made with the written informed consent of the patient. Under general anesthesia with all aseptic precautions, the patient was treated with skeletal traction to the amputation stump through a Denham pin and closed reduction of the fracture on an orthopedic traction table (Fig. 2). Closed reduction was achieved by connecting the Denham pin to the traction table with the help of a Bohler stirrup and cables. Acceptable reduction was achieved, maintained, and confirmed under Image intensifier. After this, the limb was again prepared with antiseptic solution and draped. A lateral incision was made over the proximal femur and dissection was carried out to the bone through fascia, iliotibial band, and muscle. Using a 135° angle guide, guide wire was inserted and position confirmed under image intensifier. After triple reaming over the guide wire, 75 mm Lag screw was placed along with a 4-hole DHS plate (Fig. 3 and 4). Closure was done in layers; a dressing was applied.

Postoperatively, the patient was allowed to mobilize weight bearing on the operated limb as tolerated. Thromboprophylaxis was given as per hospital policy. The skin clips were removed at 2 weeks from the surgery.
Follow-up and outcome
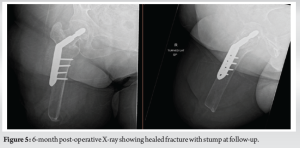
The patient was followed up at 10-week and 6-month post-operative. During the first follow-up, it was noted that the surgical site had healed well without any wound-related complications. The patient was able to weight bear on the operated limb and use it for independent transfer to and from her wheelchair. There was no pain or discomfort reported at the site of injury and surgery. At the initial follow-up, the X-ray showed satisfactory position of the implant and healing fracture. At the subsequent follow-up at 6 months, the patient reported no pain at the site of injury and surgery and was back to her pre-injury function. She was encouraged to return to her pre-injury routine including restarting recreational activities. Radiographically, the implant position was satisfactory and the fracture had healed well (Fig. 5). The overall outcome functional and radiological was satisfactory considering a well-healed fracture, satisfactory implant position, no surgical wound-related complications, and return to pre-injury function.
Intertrochanteric femur fractures are uncommon in patients having ipsilateral above-knee amputations [4]. Depending on the fracture pattern, degree of comminution, and surgeon preference, these fractures are fixed either with an intramedullary nail or a DHS [2]. Both these operations are usually done using an orthopedic traction table. Conventionally, the patient is placed supine on the operating table and the injured limb is attached securely to the traction arm by placing the foot in the boot attachment of the traction arm and securing it with fasteners and adhesive tape, bandage. Once the limb is fixed as such it can be controlled and manipulated by adjusting the traction and rotation to reduce the fracture. Adduction/abduction and elevation can also be controlled through the traction arm to aid and maintain reduction. However, in case of amputation of the ipsilateral limb either above or below knee, it is not possible to achieve this due to the absence of the entirety of the limb, thus posing a challenge to the surgeon. The contralateral limb is usually positioned in abduction or abduction with flexion of the knee in a stirrup to aid the C-arm to come in and rotate between the two limbs for adequate fluoroscopic imaging of the fracture. In cases of bilateral above-knee amputations, this becomes a further challenge in terms of positioning the patient. This can be overcome using a technique published by Jain et al. by tying the stump to the operation table in flexion and abduction and securing it with elastic bandage and adhesive tape [5]. In cases of below-knee amputation with ipsilateral intertrochanteric or intracapsular neck femur fractures, the positioning of the injured leg on the traction table is easier. Few authors have described a method of inverting the boot attachment of the traction arm to face downward and then flexing the knee and placing the stump directly in the inverted boot. Al-Harthy et al. Tanpure et al., and Ochi et al. have all shown satisfactory reduction and fixation using this method [6, 7, 8]. Rethnam et al. have described a case where they used the prosthesis fitted onto the stump and secured it to the traction boot like a normal limb with additional support underneath in the form of a radiolucent cushioned support [9]. Patients with above-knee amputations are more challenging to position on the traction table attachments and the techniques mentioned above cannot be used. Nardulli et al. have described a method eliminating the use of a traction table. They have used AO-type femoral distractors proximal and distal to the fracture to aid and maintain reduction and fixed the fracture with a DHS. This method is done on a standard radiolucent operation table without need of traction devices [10]. Skin traction through the amputation stump is another technique which is described by Lee et al. where they have connected the stump to the boot of the traction table through skin traction using adhesive tape. Although it is difficult to maintain adequate traction and rotation through skin traction alone, Lee et al. have reported satisfactory reduction using the skin traction apparatus [11]. Manual traction and rotation by an assistant directly to the stump is another way described but is inadequate for displaced fractures due to the short lever arm available in an above-knee amputation. Manual traction and rotation applied through a Schantz pin inserted below the level of the fracture were used by Jain et al. for a displaced intracapsular neck femur fracture. However, they report inadequate reduction by this method and that eventually open reduction was carried out through an anterior approach [5]. A more reliable way to apply adequate traction and rotation through the amputation stump is skeletal traction. However, it may not always be effective in controlling rotation as Takeba et al. have reported. They used a 2.4 mm K wire through the distal part of the amputated bone with a horseshoe clamp and connected it to the traction boot of the traction table. They report that although traction was adequate, the rotation had to be controlled manually by rotating the entire stump [3]. Berg et al. have reported a case where they used skeletal traction with a Steinman pin and a Bohlers stirrup connected to the traction arm with clamps. This is similar to our case wherein we used a Denham pin with a stirrup connected to the traction arm. However, in their case, Berg et al. mention that the fracture was an occult, undisplaced fracture which did not require much manipulation [12]. In our case, it was a displaced trochanteric fracture requiring significant traction and internal rotation to reduce. With the skeletal traction and Bohler stirrup assembly attached to the traction boot by a nylon rope from the skin traction kit, adequate traction and rotation were achieved to reduce the fracture and maintain reduction. If additional rotation is required, an assistant can provide the same by rotating the stirrup through the sterile drapes. The drawbacks of using skeletal traction are possibility of cut out of the pin while applying traction due to weak bone in amputated limbs. This was a consideration which is why we have used a Denham pin with central threads to hold and engage the bone better. Other concerns such as possibility of pin site infection distally, pain at pin site, and damage to neurovascular structures remain. However, meticulous pre-operative preparation and careful surgical technique will minimize any chances of these complications.
This method of using skeletal traction through a Denham pin and Bohler stirrup assembly to adequately reduce the fracture and maintain reduction is safe, effective, and reproducible and can be used by surgeons facing a similar problem.
- Intertrochanteric fractures in limbs with ipsilateral above-knee amputation is an unusual problem faced by the orthopedic surgeon
- Good stable reduction is a key to a good outcome.
- Positioning the patient and reduction of these fractures on a traction table is challenging but achievable using the techniques described in the article.
- The surgeon must understand the problems unique to the situation at hand and use the techniques discussed above to best suit the situation and resources available.
References
- 1.Pillai A, Eranki V, Shenoy R, Hadidi M. Age related incidence and early outcomes of hip fractures: A prospective cohort study of 1177 patients. J Orthop Surg Res 2011;6:5. [Google Scholar]
- 2.Sambandam SN, Chandrasekharan J, Mounasamy V, Mauffrey C. Intertrochanteric fractures: A review of fixation methods. Eur J Orthop Surg Traumatol 2016;26:339-53. [Google Scholar]
- 3.Takeba J, Imai H, Kikuchi S, Matsumoto H, Moriyama N, Nakabayashi Y. A simple method for positioning the traction table during fixation surgery for a displaced femoral trochanteric fracture in a patient following ipsilateral above-the-knee amputation: A case report. J Orthop Case Rep 2020;10:76-9. [Google Scholar]
- 4.Haleem S, Yousaf S, Hamid T, Nagappa S, Parker MJ. Characteristics and outcomes of hip fractures in lower limb amputees. Injury 2021;52:914-7. [Google Scholar]
- 5.Jain A, Bansal H, Mittal S, Kumar A, Trikha V. Intracapsular fracture of the proximal femur in a bilateral above-knee amputee: A case report with technical tips for intraoperative positioning and literature review. Chin J Traumatol 2022;25:306-10. [Google Scholar]
- 6.Al-Harthy A, Abed R, Campbell AC. Manipulation of hip fracture in the below-knee amputee. Injury 1997;28:570. [Google Scholar]
- 7.Tanpure S, Chaugule C, Date J, Naikwade D. Intertrochanteric femur fracture fixation in a patient with below-knee amputation presents a surgical dilemma: A case report. J Orthop Case Rep 2022;12:105-8. [Google Scholar]
- 8.Ochi H, Baba T, Hamanaka T, Ozaki Y, Watari T, Homma Y, et al. Safe and effective reduction technique for intertrochanteric fracture with ipsilateral below-knee amputated limb. Case Rep Orthop 2017;2017:2672905. [Google Scholar]
- 9.Rethnam U, Yesupalan RS, Shoaib A, Ratnam TK. Hip fracture fixation in a patient with below-knee amputation presents a surgical dilemma: A case report. J Med Case Rep 2008;2:296. [Google Scholar]
- 10.Nardulli CM, Issack PS. ORIF of an intertrochanteric fracture proximal to an above-knee amputation using two AO femoral distractors. Trauma Case Rep 2023;44:100806. [Google Scholar]
- 11.Lee SM, Suh KT, Oh YK, Shin WC. Manipulation of intertrochanteric fractures in patients with below- or above-knee amputation using a fracture table: Two case reports. Medicine 2021;100:e24233. [Google Scholar]
- 12.Berg AJ, Bhatia C. Neck of femur fracture fixation in a bilateral amputee: An uncommon condition requiring an improvised fracture table positioning technique. BMJ Case Rep 2014;2014:bcr2013203504. [Google Scholar]





