
The innovative use of a proximal humerus locking plate in pediatric comminuted subtrochanteric femur fractures demonstrates a viable alternative for secure fixation, facilitating recovery while potentially enhancing outcomes and reducing complications associated with traditional methods.
Dr. Bharath Chand, Department of Orthopedics, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: mbharathchnad@icloud.com
Introduction: Pediatric subtrochanteric femoral fractures are uncommon, constituting only 4–10% of pediatric femoral fractures. These fractures present a significant challenge due to the strong muscular forces often resulting in malalignment, complicating treatment and reduction. This case is particularly noteworthy as it involves a comminuted subtrochanteric fracture, which is even rarer and demands advanced surgical intervention. This is one of the few reported cases of using a proximal humerus locking plate for treating a comminuted subtrochanteric femoral fracture in a pediatric patient.
Case Report: A 6-year-old girl presented with a closed injury to her left thigh resulting from a twisting injury and fall while playing. She was clinically and radiologically diagnosed with a left proximal femur comminuted subtrochanteric fracture extending into the diaphysis. She was also overweight for her age. Given the patient’s age, the comminuted nature of the fracture, and the need for early mobilization, a decision was made to treat the fracture surgically. A minimally invasive technique used a proximal humerus locking plate to stabilize the fracture. The fracture healed uneventfully, and later, implant removal was also done.
Conclusion: This case report presents a successful case wherein a proximal humerus locking plate was effectively utilized to manage a comminuted subtrochanteric femoral fracture in a pediatric patient. The innovative utilization of this implant, typically designated for proximal humerus fractures, underscores its adaptability and effectiveness in achieving secure fixation and facilitating recovery in intricate pediatric femur fractures. This strategy has the potential to significantly influence orthopedic practices by offering a feasible alternative for addressing challenging comminuted subtrochanteric fractures in children, potentially enhancing outcomes and decreasing complications linked with more traditional approaches.
Keywords: Pediatric subtrochanteric fracture, comminuted fracture, proximal humerus locking plate, minimally invasive surgery.
Subtrochanteric fractures in the pediatric age group are relatively rare, reported between 4 and 10% of pediatric femoral fractures [1, 2]. These fractures are difficult to treat because of the strong pull of the flexors, abductors, and external rotators on the proximal fragment, which usually interferes with alignment. Very few studies are dedicated to managing these fractures, and there is no consensus regarding the mainstay of treatment [2, 3]. These fractures are important and have a special concern due to their high rate of associated complications [4]. The treatments are age-specific: Infants aged 0 to 6 months are treated with a Pavlik Harness, and children from 6 months to 5 years are treated with a hip spica cast. The real dilemma arises when the child is around 6 years old. There is a high association of complications with titanium elastic nails (TENS) in proximal femur fractures, so most of these fractures favor plating rather than TENS [4-7].
A 6-year-old child had an alleged history of a twisting injury and a fall while playing. This resulted in a closed injury to her left thigh region, and she complained of pain in the same region. On careful clinical examination, the limb was shortened and externally rotated, there was swelling and tenderness over the proximal aspect of the thigh, and the range of movements at the hip and knee could not be assessed. There was no distal neurovascular deficit. A plain radiograph of the pelvis with both hips and a full-length radiograph of the femur with anteroposterior and lateral views was taken (Fig. 1a and b). The child was diagnosed with a left proximal femur comminuted subtrochanteric fracture with extension into the proximal diaphysis. The fracture was identified as a subtrochanteric fracture, located within 10% of the total femur length below the lesser trochanter. The fracture was distal to the greater trochanter apophysis, comminuted with a large medial wedge fragment distal to the greater trochanter. The child was put on temporary skin traction.
Pre-operative plan
The child was planned for an operative fixation, given the age of the child being 6 years, the comminuted nature of the fracture, the location of the fracture being at the junction of metaphysis and diaphysis, and the need for early mobilization. She was also overweight for her age. Normally, TENS fixation is recommended for femur shaft fractures between the ages of 5 and 11. However, TENS will not provide adequate fixation for proximal femur fractures as it would not have sufficient proximal hold. Hence, the implant of choice would be a plate device. Pediatric proximal femur locking plates are not easily available. To obviate cost, other types of plates needed to be used. The implant options included in the plan were proximal tibia 3.5 mm posteromedial long plates, 3.5 mm long locking compression plates, proximal humerus locking plates, and 3.5 mm distal radius long locking plates.

Surgical technique
The patient was put under anesthesia and placed on a fracture table with traction in the supine position to restore length and rotation. Using an image intensifier, the apophysis of the greater trochanter was identified, and the fracture extension was shown just below the apophysis. The level of the apophysis was marked on the skin using a marker. The comminuted segment was also marked along with the segment of the femur distal to the fracture for an adequate number of screws. Then, skin incisions were made below the marked apophysis at the fracture site and distal to the fracture site. The soft tissues were then dissected. The Cobbs retractor was passed submuscularly from the proximal incision site, and the soft tissues were dissected distally to the fracture (Fig. 2). The fracture site was reduced percutaneously. Under the image intensifier, the reduction was checked and found to be satisfactory. After obtaining adequate reduction, the contour of the bone was matched with available plate options, and the eight-holed proximal humerus locking plate was found to be appropriate. The plate’s position was distal to the apophysis of the greater trochanter, and caution was taken not to injure the same. The plate was fixed proximally using four locking screws and distally with one locking and three cortical screws. Biological fixation was achieved. The wounds were closed without a drain. In the immediate post-operative period, pulses were felt equally on both sides.
Post-operative period
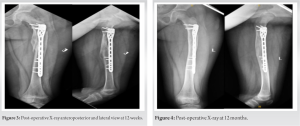
Postoperatively, the child was not mobilized due to the child’s high body mass index. In the immediate post-operative period, the child was mobilized in bed and started on knee bending, isometric quadriceps, and hamstring exercises. The child was followed up every 2 weeks, and there was progressive improvement in the knee’s range of movements. There were no wound site complications, and the wound had healed completely. A follow-up radiograph was obtained at 6 weeks and 12 weeks (Fig. 3) after the surgery. The child was started on partial weight-bearing mobilization after 6 weeks and full weight-bearing mobilization after 12 weeks postoperatively. After 12 weeks, there was a full range of movement in the knee equal to that of the opposite knee. An active straight leg raising test could be performed and no significant limb length discrepancy was noted. She has been on regular follow-ups since then (Fig. 4). She underwent an uneventful implant exit at the end of 18 months (Fig. 5).
Pediatric subtrochanteric fractures exhibit instability attributed to the muscular forces exerted on the proximal fragment. Age is the pivotal criterion determining the course of treatment for such fractures. In instances involving patients under the age of 5 years, immobilization using either a Pavlik harness or hip spica cast represents the preferred mode of treatment. Within the 6–12 age bracket, treatment modalities are at the discretion of the operating surgeon, with no universally recognized treatment protocols established for this age range. Nevertheless, opting for non-operative management increases the risk of malalignment. Extended immobilization and application of 90/90 skeletal traction are contraindicated in children with higher body weights and are correlated with an increased likelihood of shortening [8]. The operative management includes internal and external fixation. The internal fixations include intramedullary nails and plating. Even though good results were achieved with external fixators, the rate of pin tract infections is relatively high, along with loss of reduction [9]. The pin placement over the proximal fragment is also often difficult due to the location of the fracture. TENS nail is the treatment of choice due to its early weight bearing, as this nail is a load-sharing device, and healing is good with low rates of malunion and non-union. Disadvantages of TENS nails include poor rotational stability, backing out of the implant, not being suitable for comminuted fractures, the complication rate is often higher [4-7], and frequently requires a period of immobilization if the stability of the fracture is not achieved. Plate fixation can be done in a comminuted fracture to avoid complications such as shortening and rotational malalignment. The disadvantages of plate fixation include a scar, higher blood loss, overgrowth, refracture after removal, and selection of an appropriate implant. Most of the earlier studies used dynamic compression plates [10]. The child was 6 years old, obese for her age, with a proximal femur subtrochanteric comminuted fracture, not suitable for TENS and regular 3.5 dynamic/locking plating. The fracture pattern was a long spiral near the proximal femur apophysis with a shortening of 3 cm. Hence, the patient was planned for plate osteosynthesis, as the other management methods were unsuitable. The options for the same were adult proximal humerus long plates and posteromedial plates of the proximal tibia. We planned for minimally invasive percutaneous plate osteosynthesis due to the comminuted nature of the fracture and to achieve relative stability for the same. Schwarz et al. [11] followed a standard protocol of primary non-operative management for pediatric subtrochanteric fractures and dynamic compression plating for secondary osteosynthesis when fracture reduction could not be achieved with traction. Ireland and Fisher’s [3] recommendation supports conservative management using 90–90 traction and delayed spica casting in children under 10 and considering secondary operative stabilization for patients older than 10 years only if achieving satisfactory alignment through non-invasive methods is unattainable. The advantage of using a proximal humerus locking plate is it can be applied submuscularly using minimally invasive percutaneous plate osteosynthesis. In addition, complications such as periosteal stripping and vascular damage can be prevented. If other factors, such as low body mass index and intraoperative fracture stability, are achieved, early mobilization can be advised. We used an eight-holed proximal humerus locking plate due to the comminuted nature of the fracture and employed a minimally invasive biological technique to fix the plate with less stripping of the soft tissue. Due to the higher body mass index, weight bearing was delayed for 6 weeks. Initially, partial weight bearing was started at 6 weeks, followed by full weight bearing after the 12-week post-operative period. She has been on regular follow-ups since then and has had no complaints or significant limb length discrepancy of the ipsilateral lower limb. She underwent removal of the implant 18 months following fixation. Post-removal, she was allowed full weight bearing but asked to restrict sports activities for 3 months to prevent refractures due to stress shielding.
A proximal humerus locking plate can be an ideal implant for comminuted subtrochanteric pediatric femur fractures using a minimally invasive biological technique.
The use of a proximal humerus locking plate for minimally invasive percutaneous plate osteosynthesis provides an effective and adaptable solution for treating pediatric comminuted subtrochanteric femur fractures, promoting secure fixation, early mobilization, and reduced complications
References
- 1.Daum R, Jungbluth KH, Metzger E, Hecker WC. Results of treatment of subtrochanteric and supracondylous femoral fractures in children. Chirurg 1969;40:217-20. [Google Scholar]
- 2.Segal LS. Custom 95° condylar blade plate for pediatric subtrochanteric femur fractures. Orthopedics 2000;23:103-7. [Google Scholar]
- 3.Ireland DC, Fisher RL. Subtrochanteric fractures of the femur in children: Clinical orthopaedics and related research. Clin Orthop Relat Res 1975;110:157-66. [Google Scholar]
- 4.Sink EL, Gralla J, Repine M. Complications of pediatric femur fractures treated with titanium elastic nails: A comparison of fracture types. J Pediatr Orthop 2005;25:577-80. [Google Scholar]
- 5.Li Y, Heyworth BE, Glotzbecker M, Seeley M, Suppan CA, Gagnier J, et al. Comparison of titanium elastic nail and plate fixation of pediatric subtrochanteric femur fractures. J Pediatr Orthop 2013;33:232-8. [Google Scholar]
- 6.Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8. [Google Scholar]
- 7.Flynn JM, Luedtke L, Ganley TJ, Pill SG. Titanium elastic nails for pediatric femur fractures: Lessons from the learning curve. Am J Orthop (Belle Mead NJ) 2002;31:71-4. [Google Scholar]
- 8.Reeves RB, Ballard RI, Hughes JL. Internal fixation versus traction and casting of adolescent femoral shaft fractures. J Pediatr Orthop 1990;10:592-5. [Google Scholar]
- 9.Gregory P, Pevny T, Teague D. Early complications with external fixation of pediatric femoral shaft fractures. J Orthop Trauma 1996;10:191-8. [Google Scholar]
- 10.Ward WT, Levy J, Kaye A. Compression plating for child and adolescent femur fractures. J Pediatr Orthop 1992;12:626-32. [Google Scholar]
- 11.Schwarz N, Leixnering M, Frisee H. Treatment results and indications for surgery in subtrochanteric femur fractures during growth. Aktuelle Traumatol 1990;20:176-80. [Google Scholar]





