
Surgical management should be offered to patients with distal clavicle fracture and ACJ pseudo-dislocations to prevent future deformity. We recommend arthroscopic management in such cases as this surgery is intended for cosmetic purpose.
Dr. Sreejith Thampy, Department of Orthopedic Surgery, Bangalore Shoulder Institute, Bangalore, Karnataka, India. E-mail: jsthampy@gmail.com
Introduction: Acromioclavicular joint injuries are common injuries around shoulder and comprise around 9–12% and are rare in pediatric population. Many surgeries have been described which include open stabilization, arthroscopic assisted, or complete arthroscopic. We describe our technique of arthroscopic-assisted fixation in AC joint acute injuries, in which we arthroscopically pass fiber tape and tunnels across coracoid base and clavicle to stabilize the upward forces, followed by double breasting for AC joint with fiber tape to balance the horizontal forces.
Case Report: A 9-year-old female kid with a history of falls with left shoulder pain and diagnosed with fracture dislocation of the left ac joint. The patient in beach chair position. Arthroscopically, fibertape was passed through a drill hole near to cc ligament and cinch loop was done through it and around coracoid. With a mini-incision, AC joint further stabilized.
Conclusion: Similar case reports are very few and arthroscopic management of same is nearly none. Advantages of our procedure are relatively low cost of the implant, and no anchors or metal implants at AC joint to avoid impingement. Open AC joint stabilization addresses the disc in joint. Disadvantages are a long learning curve.
Keywords: Pediatric AC joint, acromioclavicular joint dislocation, arthroscopic AC joint, AC joint internal bracing, acute AC joint dislocation.
AC joint injuries comprise around 9–12% of all injuries of the shoulder and are rare in pediatric population [1]. The worldwide literature relating to this injury in pediatric patients is limited, with few cases or reports [2, 3]. Here, we describe our experience in making the diagnosis and indicating the treatment for the same. A 9-year-old girl with the left shoulder pain following a h/o fall was diagnosed with fracture dislocation of the left AC joint (Nenopoulos Group IIB, Type IV Dameron and Rockwood). Surgical fixation was done using fiber tape (2 mm) and tunnels drilled arthroscopically across the coracoid and clavicle to stabilize the vertical forces along with double-breasting for the AC joint (mini-open) to balance the horizontal forces. These injuries are rare and there are no standardized techniques or algorithms (Fig. 1).
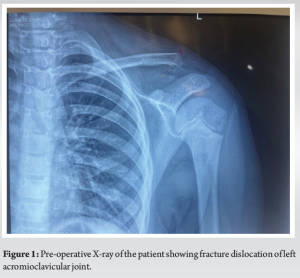
On examination, the distal end of the left clavicle showed superior displacement with tenderness over ACJ and distal clavicle, and active movement of the shoulder was painfully restricted. The skin was not threatened, and neurovascular status was normal. This was her non-dominant hand. Plain radiographs showed Group IV (classification of Nenopoulos et al.) displacement [4]. Based on these findings, the patient was diagnosed with a rare case pattern including both a distal clavicle fracture and rupture of the coracoclavicular ligaments.
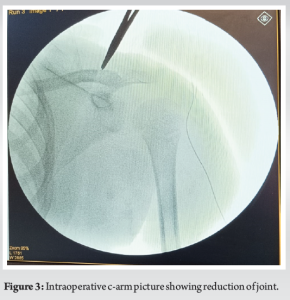
Patient was under general anesthesia and regional block and positioned in the beach chair position. Portals used include a standard posterior portal (A) and working through the anterior portal (E), the lateral end of clavicle was prepared, and an anterolateral low portal (J) created using a spinal needle. Viewing through the J portal, a mid-axillary portal (I) was created, outside in, using spinal needle, and Antero medial low port (M) created under vision. Viewing through I port and working portal through M port pectoralis minor was released, and medial and under surface of coracoid prepared. Through H port coracoid base was targeted with a drill sleeve and drilled hole created at the center of the base of coracoid near to cc ligament attachment with a 3.2 mm drill. Spinal needle along with PDS suture was passed through the drill hole. PDS suture was withdrawn through the M portal. Arthrex fiber tape was shuttled with loop inferior and free end superior. With viewing port as I port, through the M port the two free end of the fiber tape were separately retrieved and a cinch loop done in coracoid (Fig. 2). A 4 cm incision was given over clavicle and targeting a isometric point on the posterior border of clavicle which was in line to the coracoid, clavicle was drilled in a posterosuperior to anteroinferior direction. The free fiber tape ends were retrieved through the clavicle tunnel. The AC joint was reduced under c arm guidance (Fig. 3), and reduction secured with knots. The AC joint was further exposed and using a tunnel longitudinally at acromion, fiber tape was looped across the tunnel, and knot was put to stabilize AC joint additionally to counteract horizontal forces acting on the joint (Fig. 4).


Postoperatively, plain radiographs showed a well-reduced fracture with anatomical ACJ alignment. Elbow and wrist mobilization was advised till 3 weeks followed by active assisted shoulder rom exercises in supine position as tolerated. At 6-week follow-up, fracture site showed callous formation (Fig. 5), started on rehabilitation, allowing full range of movement (ROM). By 3 months, she reported no functional limitations with full return to her normal activity. Following which we arthroscopically cut the fiber tapes to prevent any growth disturbance which might occur since a child is still in the growing phase. As such no consensus exists mentioning the need for same. Patient continued to have full functional activity and returned to sporting activities immediately.

Injuries to the lateral part of an immature skeleton are likely to be separation of epiphyseal-metaphyseal region of distal end of the clavicle, a “pseudodislocation” than true acromioclavicular separations [5, 6]. True ACJ dislocations are rare below 13 years of age [6]. Ligaments in children are more elastic, which makes injuries in ACJ less likely and bone is more prone to injury [7]. These fractures are associated with rupture of the coracoclavicular ligament complex which is attached to the periosteal sleeve while the clavicle displaces, creating a “banana-peeling” phenomenon [3]. If this type of injury is neglected, the formation of new bone from the ruptured periosteal envelope may lead to the development of a “Y”-shaped clavicle which is both uncomfortable and unsightly [2, 5]. Nevertheless, long-term follow-up of non-operative treatment in this injury has also demonstrated excellent results [5]. Eidman et al. reported this type of injury, as well as the later ossification near the coracoclavicular ligament region in 14 of 25 children who were thought to have a complete acromioclavicular joint dislocation. When total rupture of the CC ligaments is suspected, surgical repair can be justified to treat the deformity [3]. Considering the excellent remodeling potential, minimally displaced fractures in skeletally immature patients can be managed conservatively [8, 9]. Center of ossification of the distal epiphysis of the clavicle appears after 18 years of age; hence, controversy continues to surround treatment for displaced fractures [2]. Ogden observed duplication of the clavicle after injuries to the distal epiphysis and recommended an open reduction to prevent a “double” clavicle [2]. Similarly, Lietchti recommended open reduction and periosteal suturing [10]. Havránek recommended surgery for esthetic reasons as seven patients in his study presented with shoulder deformity [11]. Nenopoulos et al. also emphasized on the cosmetic outcome and classified these fractures from I to V and proposed treatment algorithm [4]. Surgical management described for AC joint acute injuries include Mersilene taping, Kirschner wires or Steinmann, Bosworth screw, and ligamentoplasty [5]. Recently, one author used suture anchor but with open technique [12]. In our technique of acute AC joint injury management arthroscopically, we used fiber tape and tunnels across coracoid base and clavicle to stabilize the upward forces and followed by double breasting for AC joint with fiber tape to balance the horizontal forces. Intraoperative, the fractured medial portion of the clavicle was found denuded partially from the periosteum, and the conoid and trapezoid ligaments were ruptured. Lateral segment had the epiphyseal segment which was still in continuity with a well-maintained ACJ. We used fiber tape instead of fiber wire as the later has higher cut out chance through coracoid. Even though many surgical methods are mentioned in literature, none shows inferior results in case of unstable ACJ dislocations. Whereas the resulting post-surgical scar could end up in an even worse cosmetic result, especially in those with keloid tendency justifying arthroscopic intervention, as this surgery is intended for cosmetic outcome. Degree of periosteal detachment can be assessed using MRI. Advantages of our procedure are relatively low cost of implant, no anchors, or metal implants at AC joint to avoid impingement. Opening of AC joint for stabilization addresses the disc in joint. Disadvantages are the long learning curve, coracoid tunnel will always have possibility of cut out and theoretical tunnel loosening.
ACJ pseudodislocations are rare. Surgical management should be offered to patients with distal clavicle fracture and ACJ pseudodislocations to prevent deformity. We recommend arthroscopic management in such cases as the surgery is intended for cosmetic purpose. Using a fiber tape will further reduce hardware requirement. Thus minimizing surgical assault. Our proposed arthroscopic technique with fiber tape is a rare case of fixation managed with a new and unique technique with advantage of better cosmetic outcome with minimal invasiveness with low implant cost, no anchors/metal implants.
Surgical management should be offered to patients with distal clavicle fracture and ACJ pseudodislocations to prevent future deformity. We recommend arthroscopic management in such cases as this surgery is intended for cosmetic purpose.
References
- 1.Epidemiology of Isolated Acromioclavicular Joint Dislocation. Available from: https://pubmed.ncbi.nlm.nih.gov/23431452 [Last accessed on 2023 Sep 05]. [Google Scholar]
- 2.Ogden JA, editor. Chest and Shoulder Girdle. In: Skeletal Injury in the Child. 3rd ed. New York: Springer-Verlag; 2000. p. 438-41. [Google Scholar]
- 3.Falstie-Jensen S, Mikkelsen P. Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-9. [Google Scholar]
- 4.Outcome of Distal Clavicular Fracture Separations and Dislocations in Immature Skeleton. Available from: https://pubmed.ncbi.nlm.nih.gov/21055749 [Last accessed on 2023 Sep 05]. [Google Scholar]
- 5.Delgado J, Jaramillo D, Chauvin NA. Imaging the injured pediatric athlete: Upper extremity. Radiographics 2016;36:1672-87. [Google Scholar]
- 6.Eidman DK, Siff SJ, Hugh S. Tullos Acromioclavicular Lesions in Children; 1981. Available from: https://journals.sagepub.com/doi/abs/10.1177/036354658100900304?journalcode=ajsb [Last accessed on 2023 Sep 05]. [Google Scholar]
- 7.Black GB, McPherson JA, Reed MH. Traumatic pseudodislocation of the acromioclavicular joint in children. A fifteen year review. Am J Sports Med 1991;19:644-6. [Google Scholar]
- 8.Shah RR, Kinder J, Peelman J, Moen TC, Sarwark J. Pediatric clavicle and acromioclavicular injuries. J Pediatr Orthop 2010;30 Suppl 2:S69-72. [Google Scholar]
- 9.Wilkes JA, Hoffer MM. Clavicle fractures in head-injured children. J Orthop Trauma 1987;1:55-8. [Google Scholar]
- 10.Liechti R. Frakturen der clavicula und der scapula. In: Weber BG, Brunner C, Freuler F, editors. Die Frakturbehandlung beikindern und Jugendlichen. Berlin: Springer-Verlag; 1978. p. 87-94. [Google Scholar]
- 11.Havránek P. Injuries of distal clavicular physis in children. J Pediatr Orthop 1989;9:213-5. [Google Scholar]
- 12.Acromioclavicular Joint Pseudo-dislocations with Lateral end Clavicle Fracture: A Rare Injury and Proposed Technique of Fixation. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8930306 [Last accessed on 2023 Sep 05]. [Google Scholar]








