
Conservative management of humerus shaft fracture is the most effective treatment modality for the management of humerus shaft fracture.
Dr. gourav Mazumdar, Senior resident, Department of Orthopaedic,Deen Dayal Upadhyay hospital,New Delhi, India. Email id:- Mazumdar.gourav@gmail.com
Introduction: Conservative or surgical treatment options are available for humeral shaft fractures. To pinpoint individuals who would benefit from early surgical fixation, fracture characteristics were examined. In conservative treatment, the “U” slab prevents displacement, and overriding is corrected by gravity while the patient continues to move about. Rotation is prohibited for 14 days by holding the arm immobile to the chest with the elbow flexed. The preferred course of treatment for fractures of the humeral shaft at all levels is the hanging cast.
Materials and Methods: This study was conducted at Eras Lucknow Medical College and Hospital. Forty patients with Humerus shaft fractures (HSF) who met the inclusion criteria and presented in casualty or outpatient department participated in the study. This prospective cross-sectional study was of 24 months duration. Statistical analysis: Descriptive statistical analysis was performed to calculate the mean with corresponding standard deviations (s.d.). Test of proportion was used to find the standard normal deviate (Z) to compare the difference.
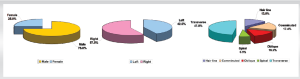
Results: The ratio of male and female (Male: Female) was 3:1. Test of proportion showed that the proportion of males (75.0%) was significantly higher than that of females (25.0%) (Z = 7.07; P < 0.001). Thus, in this study, the males were at higher risk of having fracture shaft of humerus than females. Right-sided fractures (57.5%) were significantly higher than left-sided fractures (42.5%) (Z = 2.12; P = 0.034). About 72.5% of the patients were with disabilities of the arm, shoulder, and hand (DASH) score between 14 and 16 which was significantly higher than other DASH scores (Z = 3.30; P < 0.0001).
Conclusion: Our observation regarding this study is that conservative management of HSF can be opted as the most effective way of treatment, and any complications due to any untoward event during the operative treatment should be limited.
Keywords: Humerus, displacement, fractures.
Humerus shaft fractures (HSF) are one of the most common fractures comprising approximately 3% of all fractures[1]. These fractures are categorized according to their location, openness or closure, and fracture line type. There are various techniques to deal with them although non-surgical treatment is the norm, as most humeral shaft fractures are unstable [2]. A direct impact to the upper arm causes a fracture to develop in the midshaft of the humerus. Fractures are most usually caused by trauma, such as a fall, car accident, or motorbike accident. Elderly people may also sustain this injury through falling on an extended arm, in which case the humerus suffers more damage than the wrist [3]. The middle portion of the humerus is where 60% of humeral fractures take place [4]. HSF has a non-union rate of 1–12% and require at least 4 months to recover. Transverse fractures, insufficient shoulder mobilization, and soft-tissue interposition are all linked to higher non-union rates. Conservative treatment is chosen to treat patients due to, its low cost, safety, indication for Holstein-Lewis type fractures, multiple injuries surrounding joints, and restricted mobility. Many surgeons view non-operative care as the gold standard for the management of HSF [5]. In conservative treatment, the “U” slab prevents displacement, and overriding is corrected by gravity while the patient continues to move about. Rotation is prohibited for 14 days by holding the arm immobile to the chest with the elbow flexed. The preferred course of treatment for fractures of the humeral shaft at all levels is the hanging cast [6,7]. (Fig. 1).
This study was conducted at Eras Lucknow Medical College and Hospital. Forty patients with HSF who met the inclusion criteria and presented in casualty or outpatient department (OPD) participated in the study. This prospective cross-sectional study was of 24 months duration. According to Aledanni’s study, 90.9% of the fractures healed after an average of 48 days, that is, P = 0.909. Therefore, 40.04, 40 patients were needed for this investigation to have 90% power. The following formula was used to determine sample size:
n = 4pq / (L2)
Where n = required sample size
p = 0.909 (as per the study by Aledanni)
q = 1 – p
L = Loss % (loss of information) = 10%
Calculation:
Here p = 0.909, q = 1–p = 0.091, Loss% = 10%
4pq = 4 × 0.909 × 0.091 = 0.3309
L2 = (0.909 × 0.10)2 = 0.0083
So n= 0.3309/0.0083 = 40.04 ~ 40
Inclusion criteria
Patients who had HSF within 2 weeks of the injury and who gave consent to participate in the study were taken for the surgery.
Exclusion criteria
Patients with pathological fractures, open fractures, a patient who refuses to give consent, fractures complicated by neurological and vascular damage, fractures with incomplete therapy (alternative treatment) and comorbid conditions or other injuries. After receiving treatment, patients who presented to the OPD of the ELMCH with HSF were given a data sheet to complete (according to the DASH score “The Disabilities of the Arm, Shoulder, and Hand”). DASH score:-( [{sum of n responses/n}-1] × 25).
where n is the number of completed responses
0–20% = Excellent, 21–40% = Good, 41–60% = Fair,
Above 61% = Poor
The Jawa A t al. criteria were used to grade the functional outcomes. According to the amount of range of motion (ROM) lost in either direction, shoulder and elbow function are rated as excellent, moderate, or poor. Subjective concerns like pain are also taken into consideration [8].
Grade ROM
(Shoulder/elbow) Subjective compliants
Excellent <100 loss of ROM in any direction none
Moderate Loss of ROM between 100 and 300 in any direction Mild
Poor Loss of ROM >300 in any direction Moderate-to-severe.
Statistical analysis
Statistical analysis was performed with the help of Epi Info (TM) 7.2.2.2 EPI INFO is a trademark of the Centers for Disease Control and Prevention. Descriptive statistical analysis was performed to calculate the mean with corresponding standard deviations (s.d.). Test of proportion was used to find the standard normal deviate (Z) to compare the difference.
Proportions. P < 0.05 was taken to be statistically significant.
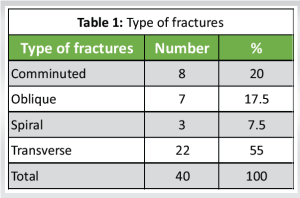
Transverse fractures (55.0%) were significantly higher than other types of fractures (Z = 5.43; P < 0.0001). Table 1.
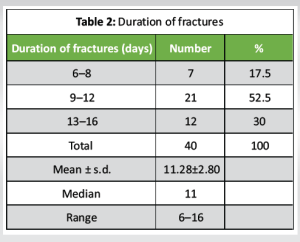
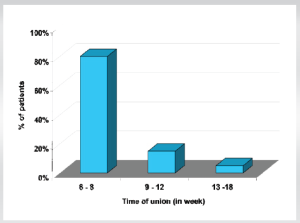
About 70.0% of the patients reported within 12 days after the fractures which was significantly higher than other duration (Z = 5.65; P < 0.0001). Table 2.
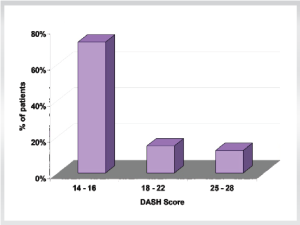
About 72.5% of the patients were with DASH score between 14 and 16 which was significantly higher than other DASH scores (Z = 3.30; P < 0.0001).
None of the patients had open reduction and internal fixation (ORIF). Dermatitis developed in only 2 (5.0%) cases. (Fig. 2,3).
In the present study, we tried to find out outcome of conservatively managed case of HSF. This study was conducted in the Department of Orthopedics, Eras Lucknow Medical College and Hospital, Lucknow. A total of 40 patients presenting to the OPD of ELMCH with HSF were treated conservatively with cast/bracing fracture. Surgical management is recommended for patients with neurovascular injuries, medullar or brachial plexus injuries, open fractures, with multiple fractures or by trauma injuries, floating elbow, and unsatisfactory reductions [8, 9, 10]. HSF can also be treated surgically for the following indications: Arbeitsgemeinschaft für Osteosynthesefragen-orthopedic trauma association Type A fractures, proximal third oblique fractures, and distal third shaft fractures [11, 12, 13]. Sandhu et al. in their study compared the functional outcomes of humerus fractures managed by conservative method versus operative procedures in reference to radiological evidence of bony union, final functional outcome, and complications. In their study, average patient age in the non-operative group was 37.4 ± 9.8 years and 37.9 ± 14.02 years in the operative group (P = 0.59) [14]. Sex distribution of the present study reveals that the ratio of male and female (Male: Female) was 3:1. Test of proportion showed that the proportion of males (75.0%) was significantly higher than that of females (25.0%), (Z = 7.07; P < 0.001). Thus in this study, the males were at higher risk of having fracture shaft of humerus than females. Laterality of the fracture in the present study reveals that right-sided fractures (57.5%) were significantly higher than left-sided fractures (42.5%) (Z = 2.12; P = 0.034). In terms of type of fracture, we found transverse fractures (55.0%) were significantly higher than other types of fractures (Z = 5.43; P < 0.0001). Regarding the interval between fracture and treatment, we found that 70.0% of the patients reported within 12 days after the fractures which was significantly higher than other duration (Z = 5.65; P < 0.0001). About 72.5% of the patients were with DASH score between 14 and 16 which was significantly higher than other DASH scores (Z = 3.30; P < 0.0001). In 77.5% of the cases, functional assessment score was excellent which was significantly higher than moderate score (22.5%) (Z = 7.63; P < 0.0001). Most of the unions (80.0%) occurred within 8 weeks which was significantly higher than union occurred beyond 6 weeks (20.0%) (Z = 8.48; P < 0.0001). None of the patients was ready ORIF. Dermatitis developed in only 2 (5.0%) cases. All humeral fractures need an assessment before opting the conservative or operative management depending on patient expectations and characteristics of fractures and conservative management can be opted successfully as an effective method of treatment in humeral shaft fracture [14]. Based on the above discussion, we can suggest that goals of humeral shaft fracture management are to establish union with an acceptable humeral alignment and put back the patients to their prior level of function. Our observation supports good results, and we can conclude that conservative management of humeral shaft fracture can be opted as the most effective way of treatment.
A total of 40 patients presenting to the OPD of ELMCH with shaft humerus fracture and were treated conservatively with after meeting the inclusion and not having any of the exclusion criteria. Regarding the age incidence of the humerus shaft fracture in the present study, we found that 70.0% of the patients were with age between 21 and 50 years which was significantly higher than other ages (Z = 5.65; P £ 0.0001). The mean age of the study participants was 34.88 ± 14.68 years. Thus, in this study, fracture shaft of humerus was more prevalent among the youngsters with working age group (aged between 21 and 50 years). Sex distribution of the present study reveals that the ratio of male and female (Male: Female) was 3:1. Test of proportion showed that proportion of males (75.0%) was significantly higher than that of females (25.0%), (Z = 7.07; P < 0.001). Thus, in this study, the males were at higher risk of having fracture shaft of humerus than females. Laterality of the fracture in the present study reveals that right-sided fractures (57.5%) were significantly higher than left-sided fractures (42.5%) (Z = 2.12; P = 0.034). In terms of type of fracture, we found transverse fractures (55.0%) were significantly higher than other types of fractures (Z = 5.43; P < 0.0001). Regarding the interval between fracture and treatment, we found that 70.0% of the patients reported within 12 days after the fractures which was significantly higher than other duration (Z = 5.65; P < 0.0001). About 72.5% of the patients were with DASH scores between 14 and 16 which was significantly higher than other DASH scores (Z = 3.30; P < 0.0001). In 77.5% of the cases, functional assessment score was excellent which was significantly higher than the moderate score (22.5%) (Z = 7.63; P < 0.0001). Most of the unions (80.0%) occurred within 8 weeks which was significantly higher than union occurred beyond 6 weeks (20.0%) (Z = 8.48; P < 0.0001). None of the patients had ORIF. Dermatitis developed in only 2 (5.0%) cases.
At the end of the study, we come to the conclusion that: Our observation regarding this study is that conservative management of HSF can be opted as the most effective way of treatment, and any complications due to any untoward event during the operative treatment should be limited.
Conservative management of humeral shaft fractures, using a “U” slab and hanging cast, offers an effective and reliable treatment option with favorable functional outcomes, particularly for patients where surgical risks are high or when surgical intervention is not immediately necessary. The study highlights that conservative treatment can significantly reduce the risk of complications associated with operative procedures, and achieve satisfactory recovery, especially in cases where proper patient selection and fracture management are applied. This approach should be considered as a first-line treatment in suitable patients to avoid surgical complications.
References
- 1.Smolle MA, Bösmüller S, Puchwein P, Ornig M, Leithner A, Seibert FJ. Complications in humeral shaft fractures - non-union, iatrogenic radial nerve palsy, and postoperative infection: A systematic review and meta-analysis. EFORT Open Rev 2022;7:95-108. [Google Scholar]
- 2.Overmann AL, Colantonio DF, Wheatley BM, Volk WR, Kilcoyne KG, Dickens JF. Incidence and Characteristics of Humeral Shaft Fractures After Subpectoral Biceps Tenodesis. Orthopaedic Journal of Sports Medicine. 2019;7(3).1-7. . [Google Scholar]
- 3.Hu B, Liu XW, Huang JJ. Surgical treatment for distal humerus type C fractures. Zhongguo Gu Shang 2018;31:976-82. [Google Scholar]
- 4.Bergh C, Wennergren D, Möller M, Brisby H. Fracture incidence in adults in relation to age and gender: A study of 27,169 fractures in the Swedish Fracture Register in a well-defined catchment area. PLoS One 2020;15:e0244291. [Google Scholar]
- 5.Leiblein M, Verboket R, Marzi I, Wagner N, Nau C. Nonunions of the humerus - treatment concepts and results of the last five years. Chin J Traumatol 2019;22:187-95. [Google Scholar]
- 6.Sarmiento A, Kinman PB, Galvin EG, Schmitt RH, Phillips JG. Functional bracing of fractures of the shaft of the humerus. J Bone Joint Surg Am 1977;59:596-601. [Google Scholar]
- 7.Rommens PM, Verbruggen J, Broos PL. Retrograde locked nailing of humeral shaft fractures. J Bone Joint Surg I995;77-B:84-9. [Google Scholar]
- 8.Jawa A, McCarty P, Doornberg J, Harris M, Ring D. Extra-articular distal-third diaphyseal fractures of the humerus. A comparison of functional bracing and plate fixation. J Bone Joint Surg Am 2006;88:2343-7. [Google Scholar]
- 9.Bell MJ, Beauchamp CG, Kellam JK, McMurty RY. The results of plating humeral shaft fractures in patients with multiple injuries: The Sunnybrook experience. J Bone Joint Surg Br 1985;67:293-6. [Google Scholar]
- 10.Dabezies EJ, Banta CJ, Murphy CP, d’Ambrosia RD. Plate fixation of the humeral shaft for acute fractures, with and without radial nerve injuries. J Orthop Trauma 1992;6:10-3. [Google Scholar]
- 11.Heim D, Herkert F, Hess P, Regazzoni P. Surgical treatment of humeral shaft fractures—the Basel experience. Journal of Trauma and Acute Care Surgery. 1993 Aug 1;35(2):226-32. [Google Scholar]
- 12.Sarmiento A, Kinman PB, Galvin EG, Schmitt RH, Phillips JG. Functional bracing of fractures of the shaft of the humerus. J Bone Joint Surg Am 1977;59:596-601. [Google Scholar]
- 13.Balfour GW, Marrero CE. Fracture brace for the treatment of humerus shaft fractures caused by gunshot wounds. Orthop Clin North Am 1995;26:55-63. [Google Scholar]
- 14.Sandhu KS, Bakshi AS, Banga RK, Kahal KS, Langeh S. Functional outcomes in humeral shaft fractures conservative management versus operative procedure. IJOS 2018;4:243-6. [Google Scholar]








