
Primary open repair of bilateral quadriceps tendon ruptures can restore knee function and lead to satisfactory outcomes.
Dr. Baibhav Mishra, Department of Orthopaedics, Ground Floor, D Block, All India Institute of Medical Science, Deoghar - 814152, Devipur, Jharkhand, India. E-mail: baibhav2100@gmail.com
Introduction: Quadriceps tendon rupture is a traumatic injury where the quadriceps detaches from the patella, disrupting the knee’s extensor mechanism. Bilateral ruptures, first documented in 1949, are rare, with an incidence of 0.17–2.5% Diagnosis involves a clinical examination, revealing a palpable defect above the patella and inability to perform a straight leg raise. Risk factors include metabolic disorders, rheumatoid arthritis, connective tissue diseases, and steroid use. In younger patients, it often results from direct trauma. Magnetic resonance imaging is the preferred diagnostic tool. While partial tears may be managed non-operatively, surgical repair is typically required for complete disruption of the extensor mechanism.
Case Report: A young man presented with an inability to walk for 1 month after a fall. He was diagnosed with bilateral quadriceps tendon rupture. Primary open repair was performed, followed by the application of bilateral long knee braces. The patient was advised delayed weight-bearing and initiated on quadriceps strengthening exercises.
Conclusion: After 12 months of follow-up, the patient showed significant improvement in function and range of motion compared to preoperative status. Primary open repair of bilateral quadriceps tendon ruptures proved to be an effective treatment, leading to satisfactory recovery and a return to good functional outcomes.
Keywords: Bilateral, quadriceps tear, primary open repair, extensor mechanism, transosseous tunnels.
Quadriceps tendon rupture is a traumatic injury where the quadriceps tendon detaches from the patella, disrupting the knee’s extensor mechanism. Bilateral ruptures, first reported in 1949, are particularly rare, with an incidence of 0.17–2.5% [1, 2]. Diagnosis is primarily clinical, identified by a palpable defect above the patella and the inability to perform a straight leg raise (active straight leg raise). Risk factors include metabolic disorders, rheumatoid arthritis, steroid use, and connective tissue disorders. In younger patients, direct trauma is the usual cause [3]. Treatment options depend on the severity: Partial tears may be managed conservatively, while complete ruptures with extensor mechanism disruption typically require surgical repair. Magnetic resonance imaging (MRI) is the preferred diagnostic tool, especially when there is uncertainty, as it helps distinguish between partial and complete tears [4]. This imaging modality is essential in confirming the diagnosis and guiding treatment decisions.
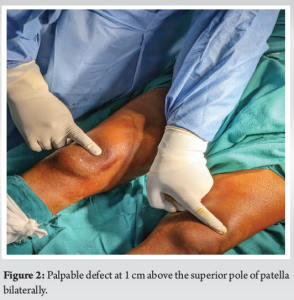
A 22-year-old man presented with complaints of inability to walk on both his legs following a direct injury to both his knees after a fall from stairs. The patient landed directly on his flexed knees rendering him unable to stand. There was bilateral loss of knee extension and active straight leg raise on examination. A palpable gap was found just above both patellae (Fig. 1). On investigation, X-rays showed bilateral patella baja and calcified masses just above the patella. MRI showed a bilateral quadriceps tear with a gap of approximately 1 cm (Fig. 2).

After evaluating the patient, primary open repair of the bilateral quadriceps tendon was planned using the trans-osseous tunnel technique, the gold standard for this condition [5]. A midline knee incision was made with tourniquet support, followed by meticulous soft-tissue dissection. The fibrosed distal stump of the quadriceps tendon was carefully removed from the superior pole of the patella. The proximal tendon was then secured to the inferior pole using a locking Krakow technique. High-tensile, non-absorbable monofilament sutures (Ethibond 5) were passed through three parallel longitudinal tunnels drilled into the patella with K-wire assistance. The wound was closed in layers (Fig. 3).

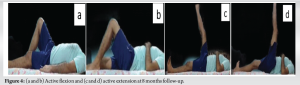
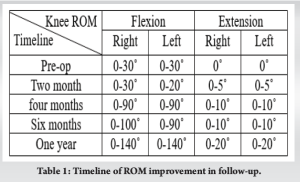
Post-surgery, the patient was placed in a hinged long knee brace in full extension. Rehabilitation began with non-weight-bearing exercises for 1 month, followed by range-of-motion exercises as tolerated for 2 months. By the 3rd month, the patient showed gradual improvement in the active range of motion, and quadriceps-strengthening exercises were introduced. At the 4-month follow-up, the patient reported significant improvement in knee pain and function. He was able to stand fully weight-bearing and walk unaided. Despite minor limitations in activities requiring greater knee strength and stability, gradually within a year, he resumed most of his daily activities with satisfactory outcomes (Fig. 4 and Table 1).
The knee extensor mechanism consists of the quadriceps tendon, quadriceps muscle, medial and lateral patellar retinacula, patella, patellar tendon, and tibial tubercle [6]. Insufficiency in any of these structures can compromise the extensor mechanism, limiting daily activities. Structurally, the quadriceps tendon is biomechanically capable of withstanding high loads without rupturing [7]. Quadriceps tendon ruptures in young non-athletes typically result from a fall, often involving knee flexion with simultaneous quadriceps contraction or extensive rotation and hyperflexion of the lower leg [8]. Although various techniques have been developed for quadriceps tendon repair, trans-osseous fixation remains the gold standard. This technique requires expertise to drill parallel longitudinal tunnels through the patella with precision, avoiding the articular surface while maintaining accurate exit holes [9]. The use of tip aimers and guidewires allows for more precise, fine tunnel drilling, reducing the risk of damaging the joint [10]. While the trans-osseous method offers advantages – such as increasing tendon-to-bone contact and promoting healing of all tendon layers – it is not recommended for patients with a patella thickness of <2 cm due to the increased risk of complications [11]. Compared to suture anchors, trans-osseous fixation has a lower pullout rate but a higher incidence of tendon displacement. Knot slippage remains the most common failure mode in both techniques, alongside other issues such as sutures tearing through tendons or breaking [12-14]. Quadriceps tendon defects may not be immediately palpable due to hematoma formation around the knee, and radiographs may not reveal fractures. In cases where the patient is lying supine with the knee in extension, the patella may not show a noticeable drop [15]. As a result, some quadriceps tendon ruptures go unrecognized for several weeks until the swelling subsides, revealing a loss of active knee extension [8]. A recent innovation by Grotting et al. is the re-tensionable suture technique, which integrates fiber tape in the trans-osseous tunnel approach. This method offers several advantages, including improved consistency of repair, as it uses a pulley and screw mechanism. However, it exposes the lower pole of the patella during the procedure [16]. It is important to note that the success of these techniques depends on the strength of the tendon, which is often compromised in cases of chronic rupture [17]. In such cases, grafts may be required. Autografts may include the gracilis or semitendinosus tendons, while allografts can include the Achilles or tibialis anterior tendons [18, 19].
Even though bilateral quadriceps tears are rare, the medical field has seen a fair share of them. With newly emerging techniques of repair, more evidence and research are needed regarding the same and the post-operative rehabilitation protocol. Although complete tears always require surgical interventions, there is always of scope for conservative treatment in case of partial tears with intact knee extensor mechanisms.
Bilateral quadriceps tendon rupture, though rare, requires high index of suspicion, especially in young patients after trauma or those with underlying metabolic or connective tissue disorders. This case emphasizes that primary open repair using the trans-osseous tunnel technique can effectively restore knee function. Postoperative management with a structured rehabilitation program, including delayed weight-bearing and gradual range-of-motion exercises, led to favorable outcomes. Early intervention and meticulous repair are crucial for optimal recovery in such complex cases.
References
- 1.Dhillon MS, Kumar P, John R, Hooda A. Bilateral quadriceps rupture in an elite weight lifter: A case report and review of literature. Indian J Orthop 2020;54:339-47. [Google Scholar]
- 2.AlShaafi WA, Alqahtani MH, Assiri AH, Alqhtani AA, Tedla JS, Motlag DS. Management of bilateral quadriceps tendon ruptures post total knee arthroplasty by kesler technique using fiber tape. Healthcare (Basel) 2023;11:631. [Google Scholar]
- 3.Zribi W, Zribi M, Guidara AR, Ben Jemaa M, Abid A, Krid N, et al. Spontaneous and simultaneous complete bilateral rupture of the quadriceps tendon in a patient receiving hemodialysis: A case report and literature review. World J Orthop 2018;9:180-4. [Google Scholar]
- 4.Dhar S. Bilateral, simultaneous, spontaneous rupture of the quadriceps tendon. A report of 3 cases and a review of the literature. Injury 1988;19:7-8. [Google Scholar]
- 5.Coladonato C, Perez AR, Sonnier JH, Looney AM, Delvadia BP, Okhuereigbe DO, et al. Similar outcomes are found between quadriceps tendon repair with transosseous tunnels and suture anchors: A systematic review and meta-analysis. Arthrosc Sports Med Rehabil 2023;5:100807. [Google Scholar]
- 6.LaPrade MD, Kallenbach SL, Aman ZS, Moatshe G, Storaci HW, Turnbull TL, et al. Biomechanical evaluation of the medial stabilizers of the patella. Am J Sports Med 2018;46:1575-82. [Google Scholar]
- 7.Barge-Caballero G, López-Bargiela P, Pombo-Otero J, Pardo-Martínez P. Quadriceps tendon rupture in wild-type transthyretin amyloidosis (ATTRwt). Eur Heart J 2019;40:1307. [Google Scholar]
- 8.Scuderi C. Ruptures of the quadriceps tendon; Study of twenty tendon ruptures. Am J Surg 1958;95:626-34. [Google Scholar]
- 9.Sherman SL, Copeland ME, Milles JL, Flood DA, Pfeiffer FM. Biomechanical evaluation of suture anchor versus transosseous tunnel quadriceps tendon repair techniques. Arthroscopy 2016;32:1117-24. [Google Scholar]
- 10.Losifidis M, Lyrtzis C, Vasiliadis AV, Metaxiotis D. Easy and safe repair of quadriceps tendon rupture through transosseous sutures: A technical note. J Arthrosc Surg Sports Med 2021;2:124-7. [Google Scholar]
- 11.Srimongkolpitak S, Chernchujit B, Apivatgaroon A, Taweekitikul P. Suture bridge transosseous quadriceps tendon repair for spontaneous quadriceps tendon rupture in patients with end-stage renal disease. Arthrosc Tech 2022;11:e2073-80. [Google Scholar]
- 12.Mehta AV, Wilson C, King TS, Gallo RA. Outcomes following quadriceps tendon repair using transosseous tunnels versus suture anchors: A systematic review. Injury 2021;52:339-44. [Google Scholar]
- 13.Belk JW, Lindsay A, Houck DA, Dragoo JL, Genuario JW, Mayer SW, et al. Biomechanical testing of suture anchor versus transosseous tunnel technique for quadriceps tendon repair yields similar outcomes: A systematic review. Arthrosc Sports Med Rehabil 2021;3:e2059-66. [Google Scholar]
- 14.Imbergamo C, Sequeira S, Bano J, Rate WR 4th, Gould H. Failure rates of suture anchor fixation versus transosseous tunnel technique for patellar tendon repair: A systematic review and meta-analysis of biomechanical studies. Orthop J Sports Med 2022;10:23259671221120212. [Google Scholar]
- 15.Kelmer GC, Johnson AH, Turcotte JJ, Bosmans ML, Redziniak DE. Tear of quadriceps and patellar tendon with superior pole avulsion of patella: A case report. JBJS Case Connect 2023;13:e22.00589. [Google Scholar]
- 16.Grotting JA, David TS, Bass S. Re-tensionable quadriceps tendon repair technique. Arthrosc Tech 2023;12: e517-21. [Google Scholar]
- 17.Alkhatatba M, Anaqreh Y, Essa SB, Alma’aiteh A, Ziad Audat H, Obeidat N, et al. Bilateral spontaneous quadriceps tendon rupture: A case report and literature review. SICOT J 2023;9:31. [Google Scholar]
- 18.Pontoh LA, Canintika AF. Reconstruction of chronic quadriceps tendon rupture using autologous semitendinosus tendon graft: A case report. Int J Surg Case Rep 2024;117:109488. [Google Scholar]
- 19.Druskin SC, Rodeo SA. Novel treatment of a failed quadriceps tendon repair in a diabetic patient using a patella-quadriceps tendon allograft. HSS J 2013;9:195-9. [Google Scholar]








