
Accurate diagnosis and differentiation of enchondroma protuberans are crucial for timely surgical intervention to prevent malignant transformation and recurrence, highlighting the need for clinical awareness and precise diagnostic protocols.
Dr. Vijay Kumar Jain, Department of Orthopaedics, Atal Bihari Vajpayee Institute of Medical Sciences, Dr Ram Manohar Lohia Hospital, New Delhi - 110001, India. E-mail: drvijayortho@gmail.com
Introduction: Enchondroma protuberans (EP), a rare form of enchondroma with exophytic growth, differs radiographically from classical enchondromas and can mimic osteochondroma, periosteal chondroma, or chondrosarcoma. Proper differentiation is crucial to avoid unnecessary radical resection, as EP requires intralesional curettage rather than the surgical removal typical for osteochondromas.
Case Report: A 14-year-old male presented with a progressively enlarging, painless mass on the lateral aspect of his left hand, initially noticed 4 years ago. Imaging and biopsy suggested osteochondroma, but histopathology confirmed enchondroma. Post-surgical excision and curettage, the patient reported no pain or limited range of motion at the 4-week follow-up.
Conclusion: Accurate diagnosis and differentiation of EP, supported by detailed radiographic and histopathological evaluation, are crucial for timely surgical intervention to prevent malignant transformation and recurrence, highlighting the need for clinical awareness and precise diagnostic protocols.
Keywords: Enchondroma, hand, cartilaginous, ollier’s disease.
Enchondromas are benign cartilaginous tumors occurring within the bony medulla that commonly occur in hand as part of Ollier’s disease or on its own [1-3]. Enchondroma protuberans (EP) is a rare form of enchondroma, with around 20 cases described in the literature to our knowledge [1]. EP is also known as ecchondroma. It shows an exophytic growth pattern that leads to deformity of the cortex, unlike classical enchondromas which are located within the intramedullary cavity [4]. Despite being a type of enchondroma, radiographically it produces images that differ from those of enchondroma. It may mimic an osteochondroma, periosteal chondroma, or chondrosarcoma [5]. To treat EP appropriately and to avoid recurrence and unnecessary radical resection, it is important to differentiate them from chondrosarcoma, periosteal chondroma, and osteochondroma. Unlike osteochondroma, which may be treated surgically by removing the cartilage cap and the stalk, EP requires intralesional curettage [6]. We describe a case of a 14-year-old male with EP of the 2nd metacarpal of the left hand with clinical, radiological, and histopathological findings.
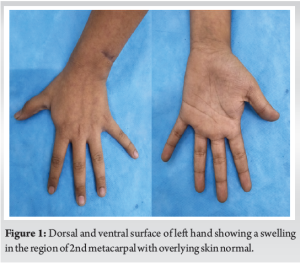
A 14-year-old male presented to the outpatient department of our hospital with a palpable mass on the lateral aspect of his left hand (Fig. 1). The patient and his family had first noticed the swelling around 4 years ago when it was small, around the size of a pea. It was painless and gradually progressed to the current size. There was no history of trauma or swelling elsewhere in the body. It was not associated with any numbness or decreased range of motion.
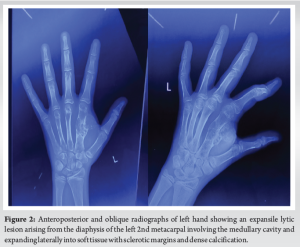
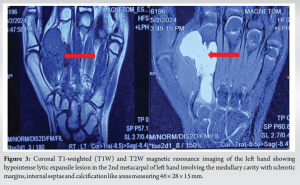
On examination, the swelling was firm to hard in consistency and did not adhere to the overlying skin but appeared to adhere to the underlying bone, hence was not mobile. The swelling was minimally tender on palpation. A radiograph of the left hand demonstrated a well-corticated expansile lesion arising from the 2nd metacarpal diaphysis and involving the medullary cavity as well (Fig. 2). Magnetic resonance imaging showed a lytic expansile lesion with an exophytic component extending laterally with a narrow zone of transition, sclerotic margins, internal calcification areas, and septae appearing hyperintense on T2 indicative of a chondroid matrix (Fig. 3). These findings were suggestive of a neoplasm of chondroid etiology, and an incisional biopsy was performed which was suggestive of osteochondroma.
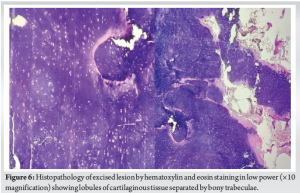
The patient was planned for surgical excision (Fig. 4), curettage, bone grafting (cortical and cancellous bone graft from ipsilateral tibia along with hydroxyapatite granules to fill the curetted cavity) (Fig. 5), and histopathological examination of the mass removed which showed lobules of cartilaginous tissue separated by bony trabeculae (Fig. 6). The chondrocytes show small round nuclei with a moderate amount of eosinophilic cytoplasm confirming the diagnosis of EP (Fig. 6). On the follow-up visit 3 weeks after the procedure, the patient reported no pain or limited range of motion and the patient stays with the regular follow-up.

Enchondromas are benign cartilaginous tumors that commonly occur in the hand and may affect any age group but are commonly seen between 10 and 30 years of age. An enchondroma is thought to originate from chondrocytes or rests of cartilage in the growth plates which separate and form columns of uncalcified cartilage under the growth plates [6]. This cartilaginous growth is usually walled off and proliferates further to form an intraosseous chondroma. Some enchondromas can, however, rarely expand through the cortex, becoming EP. Therefore, EP is a rare benign chondromatous tumor that arises in the medullary canal, forming an exophytic mass in the surrounding soft tissue. The presence of a mass is what distinguishes an EP from a classical enchondroma [1]. The most common site of EP is the hand, usually in the phalanges or metacarpal bones, followed by the ribs and the long bones of the arm [4, 7, 8]. Physical examination or clinical features as in our case are not specific or sometimes even absent. Radiographic evidence plays a key role in the pre-treatment diagnosis and helps in treatment planning considerably. On radiographs, EP appears as an expansile lytic lesion starting from the medullary cavity of the diaphysis and growing outwards into the soft tissue. There may be areas of sclerosis, sclerotic margins, and possibly dense calcifications. Based on these findings EP should be considered in the differential diagnosis of osteochondroma, chondrosarcoma, and periosteal chondroid tumours. Radiologically, EP closely resemble osteochondroma and periosteal chondroma but osteochondroma can be excluded based on the absence of a cartilage cap with underlying trabecular bone. It can be differentiated from periosteal chondroma by delineation of contiguous intramedullary involvement [9-11]. MRI is the modality of choice for EP with lesions showing cortical expansion which appear hypointense on T1 and hyperintense on T2 indicative of chondroid etiology as with our case [4]. On ultrasound EP can present as an intramedullary hypoechoic mass extending to the surrounding soft tissue through a discontinuous cortex. Punctuate or patchy calcification and blood supply may occur in some cases. However, ultrasound is not as suitable as radiographs when it comes to bony lesions [9]. A biopsy is usually done to confirm the diagnosis. On histopathology, as seen in our case, findings were lobules of cartilaginous tissue separated by bony trabeculae. The absence of nuclear atypia disorganized lobulation structure and cartilaginous cap separates it from chondrosarcoma. Treatment options available are primarily surgical. Prompt surgical treatment is advised as soon as the diagnosis is established to prevent pathological fracture of the affected bone. Definitive treatment is marginal excision with intralesional curettage to prevent recurrence because it has a rare chance of converting to chondrosarcoma. Bone grafting can be used as an adjunct [4, 11]. In our case, we did marginal, excision with intralesional curettage and bone grafting with good short-term post-operative follow-up. The patient’s symptom of pain is relieved with no restriction of range of movements.
EP underscores the importance of accurate diagnosis and differentiation, which hinges on detailed radiographic and histopathological evaluation. Prompt surgical intervention is critical to prevent potential malignant transformation and recurrence. This report contributes to the limited literature on EP, emphasizing the need for heightened clinical awareness and accurate diagnostic protocols to ensure optimal patient outcomes.
- EP, a rare benign chondromatous tumor, requires prompt surgical treatment with marginal excision and intralesional curettage to prevent recurrence and potential malignant transformation.
- Accurate diagnosis through radiographic and histopathological evaluation is crucial for effective management and favorable outcomes.
References
- 1.An YY, Kim JY, Ahn MI, Kang YK, Choi HJ. Enchondroma protuberans of the hand. Am J Roentgenol 2008;190:40-4. [Google Scholar]
- 2.Kramer HD, Valentine MJ, Pettinelli N, Kim J, Kramer RC. Ollier disease: A case report and review of treatment options. Cureus 2023;15:e43815. [Google Scholar]
- 3.Biondi NL, Tiwari V, Varacallo M. Enchondroma. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar]
- 4.Kord A, Kravis B, Rsotami S, Pandhi M, Elbaz Younes I, Bauml J. Enchondroma protuberans of the hand: A case report. Radiol Case Rep 2020;15:943-6. [Google Scholar]
- 5.Gassert FG, Breden S, Neumann J, Gassert FT, Bollwein C, Knebel C, et al. Differentiating enchondromas and atypical cartilaginous tumors in long bones with computed tomography and magnetic resonance imaging. Diagnostics (Basel) 2022;12:2186. [Google Scholar]
- 6.Crim JR, Mirra JM. Enchondroma protuberans. Report of a case and its distinction from chondrosarcoma and osteochondroma adjacent to an enchondroma. Skeletal Radiol 1990;19:431-4. [Google Scholar]
- 7.Beytemür O, Adanır O, Oncü M, Tetikkurt US. A rare cartilaginous tumor in the phalangeal bone: Enchondroma protuberans. Acta Orthop Traumatol Turc 2014;48:379-81. [Google Scholar]
- 8.Xiang X, Cheng S, Yang YJ, Qiu L. Ultrasound manifestations of enchondroma protuberans: Two case reports. Medicine (Baltimore) 2018;97:e11161. [Google Scholar]
- 9.Mohammadi A, Hedayati Asl A, Ghasemi-Rad M, Noroozinia F. Enchondroma protuberans of ulnar bone: A case report and review of literature. Case Rep Radiol 2012;2012:278920. [Google Scholar]
- 10.Dagum AB, Sampson SP. Enchondroma protuberans: A case report. J Hand Surg 1998;23:338-41. [Google Scholar]
- 11.Lasater P, Steensma MR, Patthanacharoenphon C, Davis MM. Enchondroma protuberans of the ulna in a pediatric patient: A case report. JBJS Case Connect 2016;6:e54. [Google Scholar]







